This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
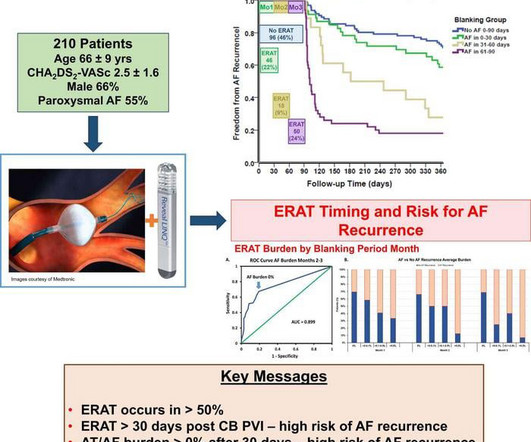
Based on continuous monitoring of early recurrence of atrial tachyarrhythmia immediately after patients have undergone atrial fibrillation ablation, Musat et al. Early recurrence of atrial tachyarrhythmia (ERAT) is commonly seen following catheter ablation of AF, with reported incidences of up to 61% in the first three months.
The unique underlying anatomic and physiological background further adds to the difficulty in eliminating the AF burden in these patients. Herein, we provide an overview of the current knowledge on the pathophysiology and risk factors for AF in adult congenital heart disease, with a special focus on the existing challenges in AF ablation.
Extensive ablation, including posterior wall isolation (PWI) is advocated for radiofrequency ablation (RFA) of persistent atrial fibrillation (peAF) to decrease the high recurrence-rates reported when only pulmonary vein isolation (PVI) is performed.1
Early recurrence of atrial arrhythmia (ERA) is commonly seen following catheter ablation of atrial fibrillation (AF), with reported incidences of up to 61% in the first three months.1 1 ERA is often attributed to transient inflammation induced by tissue damage during ablation and short-term imbalances in autonomic innervation.
By coupling AF biophysical simulations with Deep Learning (DL) algorithms, patient-specific models can be developed to predict the outcomes of various ablation strategies. However, choosing the most appropriate input features is a non-trivial task.
Atrioventricular nodal (AVN) ablation with permanent pacemaker implantation – ‘pace and ablate’ – may be considered for patients with symptomatic atrial fibrillation (AF) for whom rhythm control has been unsuccessful. Conduction-system pacing mitigates PICM, so we expect a greater uptake of AVN ablation going forward.
BACKGROUND:It is difficult to identify patients with atrial fibrillation (AF) most likely to respond to ablation. While any arrhythmia patient may recur after acutely successful ablation, AF is unusual in that patients may have long-term arrhythmia freedom despite a lack of acute success.
Recurrence rates after catheter ablation in these patients are high. Demographic, clinical, and outcome variables over 5 years were compared between patients with and without SVT recurrence.Results:Mean age of 25 patients (56% male) at time of SVT ablation was 31.5 ± 7.2 Ablation success rate was 92%.
Publication date: Available online 4 April 2025 Source: The American Journal of Cardiology Author(s): Wen Yang, Zhixin Jiang, Shengchan Wang, Chun Chen, Xiujuan Zhou, Qijun Shan
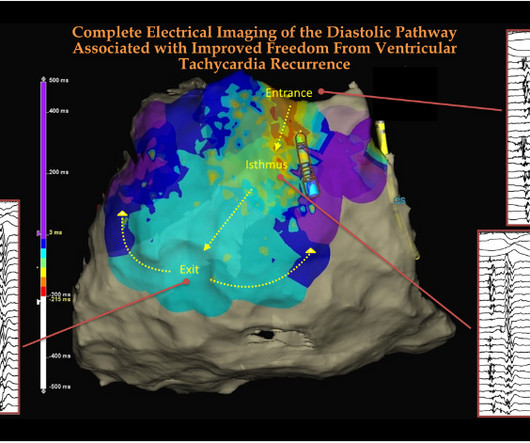
While , treating VTs with drugs is still a choice, permanent solutions by defining the VT circuit and ablating them, is the new norm. The following image and video clip is one such demonstration of ablating hidden diastolic paths between the entry and exit points. How can we remember this EP lesson easily ?
His bundle pacing (HBP) is the most physiologic pacing. In pts undergoing AV node ablation (AVNA), LBBP results in RVCD that is not correctable by fusion with native RBB conduction as achievable in pts with LBBB. However HBP threshold can be high especially in LBBB.
In the article, “Pulsed field ablation prevents left atrial restrictive physiology after posterior wall isolation in patients with persistent atrial fibrillation” by Ariel Banai and colleagues, published in the August 2024 issue of Heart Rhythm (21;8:1245-1247), the author Disclaimer information was incomplete.
Results Ablation of the rightward inferior extension was unsuccessful in eliminating DAVNNT; however, subsequent ablation of the LIE successfully eradicated the arrhythmia. Methods Diagnosis was made using adenosine triphosphate (ATP) injection during atrial pacing in a suspected DAVNNT patient.
A 50-year-old woman was referred to our hospital for catheter ablation of a regular narrow QRS tachycardia with a short RP interval. No retrograde dual atrioventricular (AV) nodal physiology was observed. In an electrophysiological study, the baseline atrio-His (AH) and His-ventricular intervals were normal.
The autonomic nervous system (ANS) is critical to atrial fibrillation (AF) pathophysiology, but it is often difficult to differentiate vagal and adrenergic AF due to complex physiological interactions.1 2 We previously reported that ERPs were associated with increased susceptibility to AF.3
This study aimed to investigate hemodynamic factors in DS generation and rupture using anatomic and ablated IA models under various DS scenarios.Methods:113 computational models of 43 patients with at least one IA containing a DS were built based on 3D rotational angiographical images using benchmarked model reconstruction procedures.
Is this patient a candidate for cardioversion or ablation? ( If ablation is contemplated — definitive diagnosis will be made at EP study. ( It simply does not make physiologic sense to suddenly see an all-negative QRS complex in this most lateral chest lead. What is the goal for treatment of this patient's AFlutter?
AV synchrony and physiologic ventricular depolarization the hemodynamics improved. Lowering the back up rate (LRL) of the ICD/pacer allowed for an intrinsic rhythm with physiologic AV conduction and normal AV synchrony with resultant increase in stroke volume and cardiac outpt.
In other cases, the bypass tracts conduct intermittently, depending upon other factors such as cardioactive medication use, physiological stressors with catecholamine release, the development of coronary ischemia, and normal aging.”[3]
Furthermore, it includes the latest recommendations which specifically address AF and thromboembolic risk assessment, anticoagulation, left atrial appendage occlusion, AF catheter or surgical ablation, and risk factor modification and AF prevention. As such, the Class of Recommendation for catheter ablation has been upgraded.
Can you ever think of ablating PVs in a patient with AF and COPD, where the right atrium is under stress and strain? (See below) It can be in the free walls of the left atrium, LA appendage, IAS, IV, SVC junctions, coronary sinus, ligament of Marshall, crista terminalis, etc.
When these measures did not work — the patient underwent PVC ablation, which did achieve a good clinical result. Learning points : Dual AV physiology in the retrograde direction does not necessarily mean there is dual AV conduction in the antegrade direction. Dual AV physiology is necessary for AVNRT and reciprocal or "echo" beats.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
























Let's personalize your content