This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Distribution Variance of Focal Atrial Tachycardia Foci and Long-Term Outcomes After Ablation. ABSTRACT Introduction The distribution of the origin of focal atrial tachycardia (FAT) in patients with different ages have not been clearly elucidated. After a mean follow-up of 47.2 months, FAT recurred in 57 patients.
Among patients with ventricular tachycardia and ischemic cardiomyopathy, catheter ablation as an initial therapy led to a lower risk of adverse outcomes than antiarrhythmic drug therapy.
BACKGROUND:Current outcomes from catheter ablation for scar-dependent ventricular tachycardia (VT) are limited by high recurrence rates and long procedure durations. Predicted optimum ablation sites to terminate all VTs in the models were identified. Circulation, Ahead of Print.
Outcomes of ablation with the FARAPULSE PFA System – a nonthermal treatment in which electric fields selectively ablate heart tissue – will be compared to outcomes following use of anti-arrhythmic drug (AAD) therapy, which is commonly prescribed for patients living with persistent AF. The company now anticipates U.S.
What are the outcomes of patients referred for ventricular tachycardia (VT) ablation according to left ventricular ejection fraction (LVEF), tolerance of VT, and acute ablationoutcome?
Abstract Introduction Some previous studies have reported that a first-step ethanol infusion into the vein of Marshall (EIVOM) with touch-up radiofrequency (RF) ablation can facilitate mitral isthmus (MI) block and improves the ablationoutcomes in persistent atrial fibrillation (PeAF) patients. 0.78, p = .006).
Patients with non-ischemic left ventricular dilated cardiomyopathy (NIDCM) and ventricular tachycardia (VT) typically have a basal perivalvular substrate adjacent with specific distribution dependent on the genetic background.1-4 1-4 Isolated apical substrate responsible for VT in NIDCM with perivalvular sparing is rare.
Twenty‐six PVT/ventricular fibrillation–triggering PVCs were identified for ablation. After a mean follow‐up of 49 months after ablation, 8 (57%) patients were free from syncope recurrence. Ablation of trigger beat significantly reduced the syncope frequency (mean±SD, 4.3±1.6
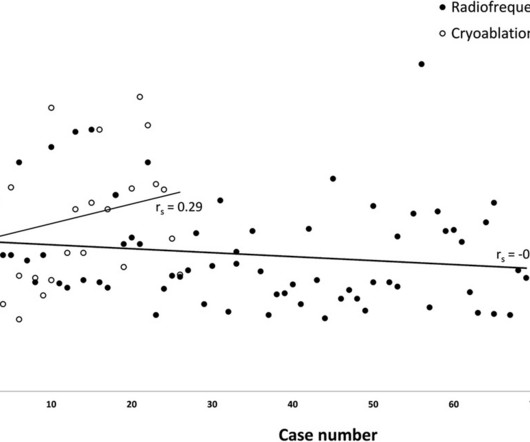
BackgroundCryoablation for pediatric atrioventricular nodal reentry tachycardia (AVNRT) is favored for reducing conduction system injury compared to radiofrequency (RF) ablation. Currently, 3D EAM systems offer precise and efficient guidance, improving safety and outcomes. Recurrence rates were 2.9% vs. 11.5%, p>0.99).
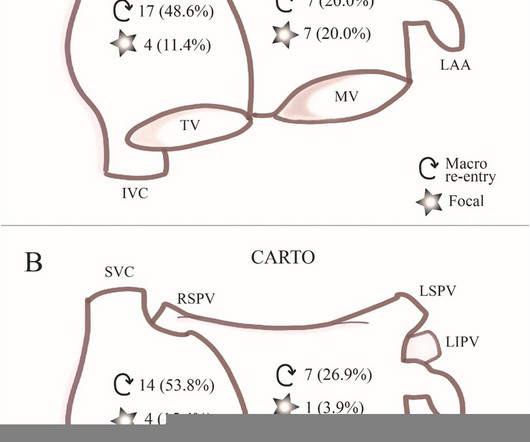
IntroductionAtrial tachycardia (AT) frequently occurs after cardiac surgery or surgical ablation procedures. The novel charge density-based mapping system (CDM) provides global chamber mapping and can detect crucial pathways of conduction; therefore, it has potential added value in catheter ablation (CA) of post-surgical ATs.
Catheter ablation is an effective tool to reduce ventricular tachycardia (VT) burden. There is a lack of robust data studying the intraprocedural characteristics and outcomes of VT ablation in patients with non-ischemic (NICM) versus ischemic cardiomyopathy (ICM).
Limited information exists regarding the effects of concurrent atrial flutter on the long-term outcomes of rhythm control. This study investigated the association between concurrent typical atrial flutter and cavotricuspid isthmus (CTI) ablation and the recurrence of atrial arrhythmia. vs. 29.9%, p < 0.001).
In the context of VT ablation, functional electroanatomic mapping techniques may help identify arrhythmogenic substrates in scarred and normal voltage areas.
The optimal timing for ventricular tachycardia (VT) ablation in reducing VT recurrence and improving patient survival is an important but unresolved topic.
Ablation of regions demonstrating spatiotemporal dispersion (SD) has been demonstrated as an alternative strategy beyond pulmonary vein isolation in patients with persistent atrial fibrillation. Occurrence of atrial tachycardia (AT) following ablation remains a limitation of this approach.
With advancements in ventricular tachycardia (VT) ablation, maintaining end-organ perfusion and hemodynamic stability is paramount. However, outcomes with its use are not well established. However, outcomes with its use are not well established.
Catheter ablation (CA) is effective in the treatment of ventricular tachycardia (VT). Although some data suggest patients with non-ischemic cardiomyopathy (NCIM) have worse outcomes compared to those with an ischemic etiology (ICM), direct comparisons are scarcely reported.
Catheter ablation is an effective therapy for ventricular tachycardia (VT) and is increasing in use. Assessment of contemporary real-world outcomes of VT ablation requires data inclusive of both inpatient and outpatient encounters.
Recurrent ventricular tachycardia (VT) can be treated by substrate modification of the myocardial scar by catheter ablation during sinus rhythm without VT induction. Better defining this arrhythmic substrate could help improve outcome and reduce ablation burden.
Earlier studies have shown regional variations in outcomes after invasive cardiovascular procedures (1). However, there is a paucity of such data concerning VT ablation in the United States.
Among patients with ischemic cardiomyopathy and ventricular tachycardia (VT), catheter ablation as a first-line strategy over antiarrhythmic drugs (AAD) was associated with a lower risk of the primary outcome, according to results of the VANISH2 trial.
There is limited data regarding safety, electrophysiologic characteristics and arrhythmia substrate during ventricular tachycardia (VT) ablation in patients with prior aortic valve replacement (AVR).
Catheter ablation for ventricular tachycardia (VT) has been shown to decrease the risk of VT recurrence and hospitalization. However, a critical gap exists in national-level data assessing its impact on hospital outcomes in patients with acute heart failure with reduced ejection fraction (HFrEF).
Stereotactic arrhythmia radioablation (STAR) is used as a rescue treatment for refractory ventricular tachycardia (VT) following unsuccessful radiofrequency catheter ablation (RFCA). The mid-term outcomes of STAR, however, remain poorly known.
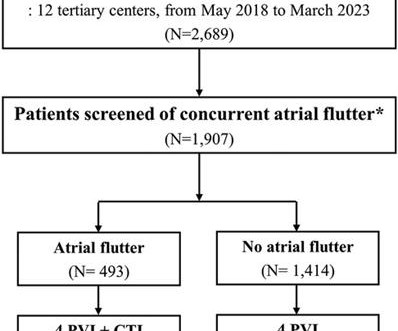
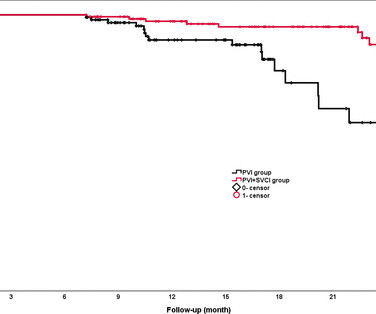
Background The value of empirical superior vena cava isolation (SVCI) following pulmonary vein isolation (PVI) to improve the efficacy of radiofrequency catheter ablation (RFCA) for paroxysmal atrial fibrillation (PAF) remains controversial. RFCA was guided by quantitative AI in both groups. vs 81.5%, p=0.02). 95% CI 0.19
Multiple risk factors for arrhythmia recurrence after Ventricular Tachycardia (VT) ablation have been identified. However, the cumulative impact of these risk factors has not been evaluated, making it challenging to predict these risks in patients with multiple coexisting conditions.
Ventricular tachycardia (VT) ablation in structural heart disease improves arrhythmia free survival. Procedural factors that influence these outcomes are not well described.
Introduction A high recurrence rate of atrial fibrillation was monitored after catheter ablation for persistent atrial fibrillation. The primary outcome will be sinus rhythm maintenance rate over 12 months, monitored by random electrocardiogram and 24-h Holter electrocardiogram.
Pulsed-field ablation (PFA) is becoming increasingly relevant in the field of electrophysiology. Data on the use is sparse, especially for atrial tachycardia (AT). Data on the use is sparse, especially for atrial tachycardia (AT).
Ventricular tachycardia (VT) is associated with significant morbidity and mortality particularly in patients with severe HF undergoing destination left ventricular assist device (LVAD) implantation. In the surgical OR, VT is difficult to map without conventional mapping equipment.
Mapping data in post-myocardial infarction (MI) patients describe ventricular tachycardia (VT) re-entry circuits of slow VT, that are typically related to transmural scars. Fast VTs with cycle lengths close to the refractory period may be related to functional re-entry in the scar border zone (BZ).
The distribution of sites of origin and long-term outcomes of focal atrial tachycardia (FAT) among patients of all ages have not been clearly explained.
Abstract Introduction The utility of ablation index (AI) to guide ventricular tachycardia (VT) ablation in patients with structural heart disease is unknown. Methods Consecutive patients ( n = 103) undergoing initial VT ablation at a single center from 2017 to 2022 were evaluated. 18], core isolation [5% vs. 11%; p = .4],
Pulsed field ablation (PFA) has become increasingly important in the treatment of cardiac arrhythmias. In addition to single-shot devices mainly used for pulmonary vein isolation, focal PFA may provide a treatment option that increases the versatility of the technique.
BACKGROUND:Epicardial approach in ventricular tachycardia (VT) ablation is still regarded as a second-step strategy, due to the risk of complications. The epicardial approach was considered useful if epicardial ablation was performed after epicardial mapping. Circulation: Arrhythmia and Electrophysiology, Ahead of Print.
ABSTRACT Introduction The aim of this study was to describe our experience and outcome of ablation therapy for arrhythmias in pediatrics at a tertiary care center. All pediatrics presenting to AUBMC between 2000 and 2020 who underwent cardiac ablation were included. Results We had 67 patients who underwent cardiac ablation.
Ablation in VT in patients with electrical storm (ES) is challenging and associated with increased peri-procedural morbidity and mortality. The implications of ES on electrophysiological characteristics are not well understood.
Cheng and Zhang to our paper1, we note that despite ARVC being a relatively uncommon cardiomyopathy, we uniquely report on a large clinical experience with very long-term follow-up after VT ablation and confirm a high incidence of atrial flutter (AFL) and the effectiveness and low risk of catheter ablation of AFL.
Wild-type transthyretin amyloid cardiomyopathy (ATTRwt-CM) is often accompanied by atrial fibrillation (AF), atrial flutter (AFL), and atrial tachycardia (AT), which are difficult to control because beta-blockers and antiarrhythmic drugs can worsen heart failure (HF).
Diastolic pathway recording has been associated with a high rate of VT termination, non-inducibility at the end of the study7 and better long-term outcome if the complete diastolic activity is recorded8. Besides the interest for functional mapping in sinus rhythm, activation mapping still plays a crucial role 1,2,3,4,5,6.
ECG data during the clinical arrhythmia (ventricular tachycardia [VT], upper left figure) is analyzed with an artificial intelligence algorithm which identifies a probable location of the source of the arrhythmia (left ventricular anterolateral papillary muscle, lower left figure). cm, LVEF 50 ± 18%) and was similar to 28 controls.
Abstract Background The newly introduced nonthermal pulsed field ablation (PFA) is a promising technology to achieve fast pulmonary vein isolation (PVI) with high acute success rates and good safety features. Compared to PFA VHPSD-PVI might ensure information on left atrial substrate allowing to target concomitant secondary tachycardias.
Abstract Introduction Despite advanced ablation strategies and major technological improvements, treatment of persistent atrial fibrillation (AF) remains challenging and the underlying pathophysiology is not fully understood. ms after) and AF termination to atrial tachycardia (AT) or sinus rhythm (SR) in 12 patients (24%).
In the past decade, major advances were made in catheter ablation for arrhythmias and implantation of cardiac implantable electronic devices.1 1 Catheter ablation for atrial fibrillation (AF) and ventricular tachycardia (VT) has become the standard of care for many patients presenting with these arrhythmias.2–4
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


































Let's personalize your content