This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Strokes and silent ischemia remain a serious complication of atrial fibrillation catheter ablation (AFCA). This is mainly due to extensive ablation lesions in the left atrium that create large areas of endothelial injury that produces prothrombotic states during and after AFCA.
Monomorphic ventricular tachycardia in the setting of acute myocardial ischemia can also be treated by intravenous lignocaine bolus followed by infusion. Predisposing causes for ventricular tachycardia like ischemia and electrolyte imbalance has to be treated simultaneously to prevent recurrence.
Is there ischemia? ECG Diagnosis is either : 1) junctional rhythm with new LBBB, and possibly ischemia 2) accelerated idoventricular rhythm with possible ischemia, and possibly related to restoration of normal perfusion. Exactly how they relate to ischemia, chest pain, and reperfusion can only be speculated about.
Are you confident there is no ischemia? Primary VT , and the VT with tachycardia is causing ischemia with chest discomfort (supply-demand mismatch/type 2 MI)? Ischemia from ACS causing the chest discomfort, with VT another consequence (or coincidence)? Do you agree with this strategy? How can you better assess the ST segments?
There is no definite evidence of acute ischemia. (ie, Simply stated — t he patient was having recurrent PMVT without Q Tc prolongation, and without evidence of ongoing transmural ischemia. ( Some residual ischemia in the infarct border might still be present. Both episodes are initiated by an "R-on-T" phenomenon.
Automatic ventricular tachycardia can occur in acute ischemia, electrolyte imbalance and with increased sympathetic tone. Radiofrequency catheter ablation is highly effective (85%-90%) in those with severe symptoms. Either case, the treatment is ablation of the right bundle. The sinus rhythm ECG can manifest an LBBB pattern.
We have previously shown that ablation of CaMKIIδ oxidation by CRISPR-Cas9 base editing enables the heart to recover function from otherwise severe damage following ischemia/reperfusion (IR) injury. Here, we extended this therapeutic concept toward potential clinical translation.
Select eSINE-RNAs were ablated via intracerebroventricular injection of antisense oligonucleotides followed by 1h MCAO and 24h reperfusion. Immunohistochemistry and RNA-FISH were used in tandem to determine the cell-type and subcellular localization of several highly expressed eSINE-RNAs.
ET Main Tent (Hall B1) This session offers more insights from key clinical trials presented at ACC.24 24 and find out what it all means for your patients.
And superimposed subendocardial ischemia pattern, of course. Is this patient a candidate for cardioversion or ablation? ( If ablation is contemplated — definitive diagnosis will be made at EP study. ( She was otherwise very stable during this rhythm. The physicians gave some IV metoprolol and restarted her on home PO metoprolol.
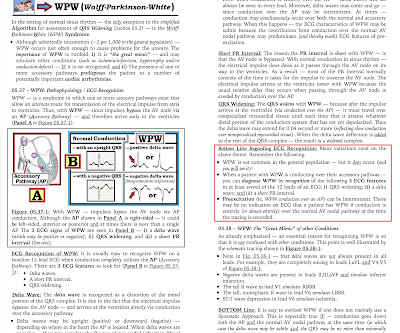
2] Conduction through the accessory pathway can be intermittent (with different degrees of pre-excitation), and affected by ischemia. 3] So a patient with WPW can have the pattern induced by ischemia, and there is also a report of a patient with pre-existing WPW which was “ablated” by myocardial infarction after an LAD occlusion.[4]
He got an MR, however that showed no scar or evidence of AVRD and he had a stress test with no evidence of inducible ischemia with almost 20 METs." It was ablated. == MY Comment , by K EN G RAUER, MD ( 6/28 /2023 ): == There is a tendency for clinicians to interpret cardiac arrhythmias in binary fashion.
A left-sided lateral wall AP was found on EP study — and successfully ablated. In addition — knowing the AP location helps in planning the EP study procedure, as well as in patient discussion — since risks of catheter ablation and likely success rates are based in part on localization of the AP.
We see a regular tachycardia with a narrow QRS complex and no evidence of OMI or subendocardial ischemia. There is no need to immediately refer today’s patient to EP for ablation. Patients should be offered a choice for a trial of medication vs ablation for this non-life-threatening arrhythmia. Her initial EKG is below.
The patient was found to have a "concealed" posteroseptal pathway (WPW without delta waves) confirmed to have SVT at EP study and was ablated. Here is the Electrophysilogist's note: "Only 1 pathway attachment could be ablated, the second one deep within the CS could not be ablated with high power.
Here is her post-cardioversion ECG: ECG#2 - Immediately post cardioversion: Appropriate ST depression maximal in V5-6 and lead II, secondary to subendocardial ischemia, likely residual from the preceding tachycardia. Radiofrequency ablation was performed for a right sided posteroseptal bypass tract. She was sedated and cardioverted.
CABG and Concomitant Ablation for Atrial Fibrillation, Left Atrial Appendage Management – How I Do It Niv Ad, MD (Silver Spring, MD, USA) 7:57 a.m. Recognizing and Managing Postoperative Myocardial Ischemia Patrick Myers (Lausanne, Switzerland) 8:23 a.m. - 8:50 a.m. Panel Discussion 8:50 a.m. – 9:50 a.m.
Relationship between Ischemia and arrhythmia While the relationship between Ischemia and VT is really complex, the term “Ischemic VT” itself adds more twists. Even here, it is the associated factors, like hypoxia or acidosis are the triggers which of course are resultant of Ischemia. Reference 1. doi: 10.1161/CIRCEP.117.006120.
Can you ever think of ablating PVs in a patient with AF and COPD, where the right atrium is under stress and strain? Hypoxic or acidotic milleu of a single atrial myocyte can iniitiate an AF, alosan episode of atrial ischemia, diffuse inflammation as in atrial epi-myocardiits can trigger AF from any spot on the atrium. Reference 1.
That said there were no clinical symptoms or ECG findings suggestive of ongoing ischemia. The patient has been scheduled for a PVC ablation procedure. Our patient was referred for EP study with a plan of PVC ablation if possible. You have given IV MgSO4 a fast acting -blocker and IV amiodarone bolus and infusion.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

























Let's personalize your content