This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
(MedPage Today) -- The efficacy of catheter ablation for heartfailure (HF) patients with atrial fibrillation (Afib or AF) hinged on the phenotype of disease, researchers reported based on a meta-analysis. Compared with conventional rate or rhythm.
Background Atrial arrhythmias (AA) and heartfailure (HF) are major causes of hospitalisation in adult congenital heart disease (ACHD). Methods In this single-centre retrospective cohort study, data from 3995 patients with ACHD were analysed.
This systematic review and meta-analysis investigates the efficacy of catheter ablation compared with rate or rhythm control among patients with atrial fibrillation and heartfailure.
Radiofrequency ablation (RFA) is an important therapeutic modality for atrial fibrillation (AF), widely utilized in clinical practice due to its safety and significant efficacy. This case report describes a unique instance of a patient developing AEF following AF ablation, accompanied by ischemic stroke and myocardial infarction.
Patients who undergo catheter ablation for atrial fibrillation (AFib) who also have heartfailure with preserved ejection fraction (HFpEF) experienced a greater benefit from ablation in terms of clinical outcome, AFib recurrence and functional status, according to findings from the CABANA trial.
It can be associated with reduced quality of life and complications such as heartfailure and stroke. Atrial fibrillation is the most prevalent arrhythmia with a lifetime risk of nearly 30%. Pulmonary vein isolation (PVI) is the most effective treatment for rhythm control.
Outcomes of ablation with the FARAPULSE PFA System – a nonthermal treatment in which electric fields selectively ablateheart tissue – will be compared to outcomes following use of anti-arrhythmic drug (AAD) therapy, which is commonly prescribed for patients living with persistent AF. The company now anticipates U.S.
Biosense Webster Study Supports Low and Zero Fluoroscopy Workflow as Safe, Effective Alternative to Conventional Catheter Ablation 5. Henry Ford Health HeartFailure Patient First in Michigan to Receive Breakthrough Device 6. Machine Learning Informs a New Tool to Guide Treatment for Acute Decompensated HeartFailure 8.
This randomized clinical trial investigates the feasibility, safety, and efficacy of endovascular right-sided splanchnic nerve ablation for volume management in heartfailure with preserved ejection fraction (HFpEF).
Atrial fibrillation catheter ablation (AFCA) improved clinical outcomes compared with medical treatment alone, and early AFCA was associated with better outcomes than late AFCA, particularly decreased risk of heartfailure (HF) hospitalization and atrial fibrillation (AFib) recurrence.
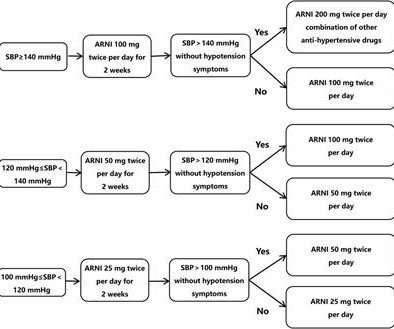
Introduction A high recurrence rate of atrial fibrillation was monitored after catheter ablation for persistent atrial fibrillation. Patients will be randomized to (1) receive the standard treatment strategy plus sacubitril/valsartan titration, or (2) receive the standard treatment strategy without taking sacubitril/valsartan.
Catheter ablation is an established and effective treatment for ventricular tachycardia (VT) in patients with heartfailure (HF). However, data on its long-term impact in heartfailure with reduced ejection fraction (HFrEF) remains scarce.
Heartfailure with preserved ejection fraction (HFpEF) is a widespread syndrome with limited therapeutic options and poorly understood immune pathophysiology. Notably, selective ablation of XBP1 in T cells enhanced their persistence in the heart and lymphoid organs of mice with preclinical HFpEF.
Predicting the anticipated benefit and selecting the optimal timing of catheter ablation of recurrent ventricular tachycardia (VT) in patients with severe heartfailure (HF) can be challenging.
American College of Cardiology (ACC) and American Heart Association (AHA) Issue New Hypertrophic Cardiomyopathy (HCM) Management Guidelines 2. New Study Published in JACC: HeartFailure Reveals that Despite Significant Efforts to Improve Acute HeartFailure Treatment Over the Past 20 Years, Management Remains Unchanged 3.
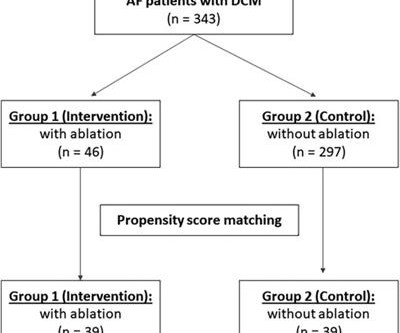
Introduction Catheter ablation is an effective and safe strategy for treating atrial fibrillation patients. Nevertheless, studies on the long-term outcomes of catheter ablation in patients with dilated cardiomyopathy are limited. Among the catheter ablation group, 58.7% ( n = 27) had persistent atrial fibrillation.
Patients with heartfailure (HF) and atrial fibrillation (AF) frequently undergo catheter ablation to maintain sinus rhythm and improve cardiovascular outcomes.
HFrEF in the presence of AF is a common clinical scenario with concerns AF recurrence will precipitate acute decompensation of heartfailure (DHF). However, the impact of AF recurrence following catheter ablation on DHF is not well understood.
Atrial Fibrillation (AF) and HeartFailure (HF) are closely interlinked. Pulsed Field Ablation (PFA) has been demonstrated to promote fast and durable Pulmonary Vein Isolation (PVI) without the risk of PV stenosis or damage to adjacent structures.
The concept of a 3-month blanking period after catheter ablation (CA) for atrial fibrillation (AF) is widely accepted. However, in AF patients with heartfailure (HF), EPR might adversely affect outcomes, though the details remain unclear.
Catheter Ablation for Atrial Fibrillation (AFib) in heartfailure is now a class I indication for patients with heartfailure. Evidence supports the relationship between obesity and the incidence and recurrence of Afib.
Rhythm control is an important strategy in managing atrial fibrillation (AF) in patients with heartfailure (HF). However, data on the long-term efficacy of catheter ablation for AF in HF remains scarce.
Atrial fibrillation (AF) is a common arrhythmia in patients with heartfailure (HF). Catheter ablation of AF has been proven to be an effective therapeutic option for AF management in HF, particularly in heartfailure with reduced ejection fraction (HFrEF) [2, 3].
Atrial fibrillation (AF) is a common reversible cause of worsening left ventricular ejection fraction (LVEF) in patients with heartfailure. Guidelines propose a class 1 recommendation for AF catheter ablation (CA) in patients with heartfailure with reduced ejection fraction1,2.
Clinical outcomes among patients with atrial fibrillation (AF) and heartfailure with preserved ejection fraction (HFpEF) treated with catheter ablation (CA) versus antiarrhythmic therapy (AAT) are not well-known.
Studies have shown detrimental effects of atrial fibrillation (AF) occurrence among patients with heartfailure (HF) with a preserved ejection fraction (HFpEF). Ablative therapy may counter this risk, but the impact of timing of ablation in paroxysmal vs. persistent AF is unclear.
AF-free survival after ablation in longstanding persistent AF (LPAF) is poor. Outcomes are worse still in LPAF patients who are overweight or obese, have heartfailure, and have significant LA dilation.
Catheter ablation for ventricular tachycardia (VT) has been shown to decrease the risk of VT recurrence and hospitalization. However, a critical gap exists in national-level data assessing its impact on hospital outcomes in patients with acute heartfailure with reduced ejection fraction (HFrEF).
Catheter ablation (CA) for atrial fibrillation (AF) and heartfailure with reduced ejection fraction <40% (HFrEF) is associated with improved outcomes. The patient characteristics, AF effect on quality-of-life questionnaire (AFEQT), and ablation strategies performed remains uncertain in those with and without HFrEF.
The efficacy of catheter ablation as a treatment approach for patients with concurrent atrial fibrillation (AF) and heartfailure with preserved ejection fraction (HFpEF) has been inadequately investigated.
Abstract A vast amount of now well-established clinical and epidemiological data indicates a close, interdependent, and symbiotic association between atrial fibrillation (AF) and heartfailure (HF). whether ablation is mandatory or pointless in patients who have HF).
Overview of the study population and effects observed after catheter ablation for atrial fibrillation. Herein we describe the effects of catheter ablation on AF burden, arrhythmia recurrences, and ventricular function in end-stage HF. to 39.18.3% ( p <0.001) following ablation. PVI, pulmonary vein isolation.
Heartfailure (HF) readmission rates remain a concern in patients with lone typical atrial flutter (AFL) and HF, even following cavo-tricuspid isthmus (CTI) ablation.
The impact of sodium-glucose cotransporter 2 inhibitors (SGLT2i) on atrial fibrillation (AF) recurrence outcomes and adverse cardiovascular outcomes in heartfailure (HF) patients after AF ablation is unknown.
Most clinical trials have suggested that strictly controlling resting heart rate (RHR) lower than 110 beats per minute (bpm) even less than 100 bpm is beneficial. However, the degree to which rate control prior to catheter ablation influence is unclear especially in AF patients with heartfailure (HF).
Catheter ablation of atrial fibrillation (AF) is the preferred strategy for improving survival and reducing heartfailure (HF) hospitalizations in patients with heartfailure with reduced ejection fraction (HFrEF) and AF.
Studies have suggested that early atrial fibrillation (AF) ablation is associated with improved outcomes. However, it is unknown whether these patterns hold for persistent AF among patients with heartfailure with preserved ejection fraction (HFpEF). The majority of these studies evaluated paroxysmal AF cases.
Previous studies have demonstrated significant morbidity and mortality in patients with heartfailure (HF) with reduced ejection fraction (HFrEF), particularly with accompanying atrial fibrillation (AF).
Research covered topics such as outcomes for pediatric subcutaneous ICD implantation; procedural success rates and risk factors associated with catheter ablation for atrial tachyarrhythmias; comparing echocardiographic guidance during left atrial appendage occlusion (LAAO); and atrial fibrillation (AFib) ablation in patients with heartfailure with (..)
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.









































Let's personalize your content