This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
(MedPage Today) -- CHICAGO -- For patients with ventricular tachycardia (VT) and ischemic cardiomyopathy, going right to catheter ablation improved outcomes compared with trying antiarrhythmic drugs first, the VANISH2 trial showed. Death or.
Among patients with ventricular tachycardia and ischemic cardiomyopathy, catheter ablation as an initial therapy led to a lower risk of adverse outcomes than antiarrhythmic drug therapy.
The goal of the VANISH2 trial was to compare endocardial catheter ablation with conventional antiarrhythmic drug (AAD) therapy as a first-line treatment for infarct-related ventricular tachycardia (VT) in ischemic cardiomyopathy.
BackgroundHypertrophic cardiomyopathy (HCM) is an autosomal dominant disorder characterized by asymmetric hypertrophy of the ventricles and the ventricular septum, leading to subsequent left ventricular outflow tract (LVOT) obstruction and diastolic dysfunction.
Implantable cardioverter defibrillator (ICD) prevents sudden cardiac death (SCD) in patients with ischemic cardiomyopathy (ICM). Catheter ablation has been shown to effectively reduce ventricular tachycardia (VT) recurrence, yet its efficacy in patients without an ICD implantation remains uncertain.
The best approach for ablating ventricular tachycardia (VT) targeting right ventricular free wall (RVFW) aneurysms in arrhythmogenic right ventricular cardiomyopathy (ARVC) remains undefined.
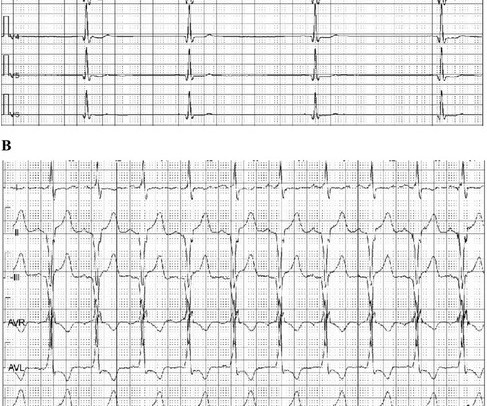
A prehospital 12-lead was recorded: There is a regular wide complex tachycardia. The computer diagnosed this as Ventricular Tachycardia. There is a wide complex regular tachycardia at a rate of 226. Toothache, incidental Wide Complex Tachycardia Could it be fascicular VT or Bundle Branch VT ( i.e., idiopathic VT )?
Patients with non-ischemic left ventricular dilated cardiomyopathy (NIDCM) and ventricular tachycardia (VT) typically have a basal perivalvular substrate adjacent with specific distribution dependent on the genetic background.1-4 1-4 Isolated apical substrate responsible for VT in NIDCM with perivalvular sparing is rare.
She had a single chamber ICD/Pacemaker implanted several years prior due to ventricular tachycardia. Answer : The ECG above shows a regular wide complex tachycardia. Said differently, the ECG shows a rather slow ventricular tachycardia with a 2:1 VA conduction. Cardiac output (CO) was being maintained by the tachycardia.
Catheter ablation is an effective tool to reduce ventricular tachycardia (VT) burden. There is a lack of robust data studying the intraprocedural characteristics and outcomes of VT ablation in patients with non-ischemic (NICM) versus ischemic cardiomyopathy (ICM).
Among patients with ischemic cardiomyopathy and ventricular tachycardia (VT), catheter ablation as a first-line strategy over antiarrhythmic drugs (AAD) was associated with a lower risk of the primary outcome, according to results of the VANISH2 trial.
A patient in the ICU with significant underlying cardiac disease [HFrEF 30%, non-ischemic cardiomyopathy, LBBB s/p CRT-D (biventricular pacer), AVNRT s/p ablation a few yrs ago, hx sinus tachycardia while on max tolerated BB therapy] went into a regular wide-complex tachycardia after intubation for severe COPD exacerbation.
Abstract Introduction Due to its unique features, pulsed field ablation (PFA) could potentially overcome some limitations of current radiofrequency (RF) ventricular tachycardia (VT) ablation. Methods Two patients with ischemic cardiomyopathy and previously failed RF VT ablations were treated with PFA.
Catheter ablation (CA) is effective in the treatment of ventricular tachycardia (VT). Although some data suggest patients with non-ischemic cardiomyopathy (NCIM) have worse outcomes compared to those with an ischemic etiology (ICM), direct comparisons are scarcely reported.
Endocardial (ENDO)-only ventricular tachycardia (VT) ablation has been found to indicate long-term VT-free survival in more than half of patients with arrhythmogenic right ventricular cardiomyopathy (ARVC) and more than 75% if VT noninducibility is achieved following ablation.
Arrhythmogenic right ventricular cardiomyopathy (ARVC) is a family inherited cardiomyopathy associated with ventricular arrhythmias. With the development of molecular biology, histology, imaging, and other dia.
Tachycardia-induced cardiomyopathy refers to changes in cardiac structure and function that result from rapid arrhythmia and can manifest as a continuous or recurrent event. Cardiomyopathy induced by atrial ta.
Cheng and Zhang to our paper1, we note that despite ARVC being a relatively uncommon cardiomyopathy, we uniquely report on a large clinical experience with very long-term follow-up after VT ablation and confirm a high incidence of atrial flutter (AFL) and the effectiveness and low risk of catheter ablation of AFL.
IntroductionFocal atrial tachycardia (FAT) is predominant in the pediatric population. A 12-lead electrocardiogram revealed a narrow QRS complex tachycardia with a rate of 157 beats per minute and a prolonged RP relationship. Echocardiography indicated a severely reduced ejection fraction of 22%.
Supraventricular tachycardias are the most common arrhythmias that occur during pregnancy. When pharmacologic therapy fails, fluoroless catheter ablation utilizing electroanatomic mapping systems and intracardiac echocardiography (ICE) may be considered. Pharmacologic therapy is often preferred in pregnant patients.
Ventricular Tachycardia (VT) is an important cause of morbidity and mortality in structural heart Disease. Current literature is limited in direct comparison of VT in ischemic (ICM) compared to non-ischemic cardiomyopathy (NICM).
Recent advancements in catheter ablation for structural ventricular tachycardia (VT), such as high-density mapping and cardiac imaging-based detection of target areas, have significantly improved the efficacy of ablation procedures.
Wild-type transthyretin amyloid cardiomyopathy (ATTRwt-CM) is often accompanied by atrial fibrillation (AF), atrial flutter (AFL), and atrial tachycardia (AT), which are difficult to control because beta-blockers and antiarrhythmic drugs can worsen heart failure (HF).
Surgical disarticulation of the right ventricular (RV) free wall has been described by Guiraudon and colleagues as an effective therapy for refractory ventricular tachycardia (VT) in arrhythmogenic right ventricular cardiomyopathy (ARVC).1
BACKGROUND:Epicardial approach in ventricular tachycardia (VT) ablation is still regarded as a second-step strategy, due to the risk of complications. The epicardial approach was considered useful if epicardial ablation was performed after epicardial mapping. Circulation: Arrhythmia and Electrophysiology, Ahead of Print.
Belhassen’s ventricular tachycardia is an uncommon arrhythmia in infants. Originating near the left posterior fascicle, it is initiated by supraventricular ectopy or sinus tachycardia and is uniquely sensitive to verapamil. Use of verapamil in infants is controversial due to risk of severe hemodynamic compromise.
Epicardial catheter ablation of ventricular tachycardia (VT) is a well-established ablation technique for a variety of myocardial substrates including ischemic cardiomyopathy. Epicardial VT ablation has several potential life-threatening complications including a 1.5% incidence of coronary artery (CA) injury.
My understanding is that the decision was made for today's patient to be formally evaluated by EP cardiology with consideration given to ablation and/or insertion of an ICD ( I mplantable C ardioverter D efibrillator ). I offer the above as retrospective reflection to stimulate discussion on actions to consider.
Atrial tachycardia (AT) originating from the left atrial appendage (LAA) is uncommon and the most difficult arrhythmia to eliminate. Therefore, we present the case of a 5-year-old girl with tachycardia-induced.
In all probability, this dilation is a form of atrial tachycardia and atrial cardiomyopathy. Spatial relationship of sites for atrial fibrillation drivers and atrial tachycardia in patients with both arrhythmias July 2017 International Journal of Cardiology 248(3) AF begets AF. Implications for electrophysiologists.
Wall thickness map derived from computed tomography angiography (CTA) has been reported to correlate with low voltage areas in patients with ischemic cardiomyopathy (ICM). The correlation between wall thinning and VT circuits has not been previously described.
Arrhythmogenic right ventricular cardiomyopathy (ARVC) is a disease characterised by fibrofatty replacement of the ventricular myocardium due to specific mutations, leading to ventricular arrhythmias and sudden cardiac death. Additionally, the impact of sotalol and amiodarone is inconsistent with studies reporting contradictory results.
They had a history of non-ischemic cardiomyopathy (EF 30%), as well as PCI with one stent. Initial ECG in the ED: Presenting ECG : Wide-complex tachycardia at a rate about 200. This is overwhelmingly likely to be ventricular tachycardia, even if only age and medical history are considered.
Ablation will be performed with the use of a substrate-based approach in which the myocardial scar is mapped and ablated while the heart remains predominantly in sinus rhythm. Cardiovascular mortality, driven by sudden cardiac death, is the main reason for dying while waiting for heart transplantation (HTx).
An 18-year-old male with arrhythmogenic cardiomyopathy was referred for catheter ablation of ventricular tachycardia after experiencing appropriate implantable cardioverter-defibrillator (ICD) shock. Six months prior, he had undergone uncomplicated implantation of an extravascular ICD (EV-ICD) [1].
Publication date: Available online 17 December 2023 Source: The American Journal of Cardiology Author(s): Hugo De Larochellière, François Brouillette, Patrick Lévesque, Nicolas Dognin, Raphaël St-Germain, Goran Rimac, Sylvain Lemay, François Philippon, Mario Sénéchal
A 72-year-old man with severe coronary artery disease (CAD) and coronary artery bypass grafting complicated by ischemic cardiomyopathy and ventricular tachycardia (VT) was referred for redo VT ablation.
Here is his 12-lead: There is a wide complex tachycardia with a rate of 257, with RBBB and LPFB (right axis deviation) morphology. Read about Fascicular VT here: Idiopathic Ventricular Tachycardias for the EM Physician Case Continued He was completely stable, so adenosine was administered. See Learning point 1 below.
Fragmented QRS is a marker of myocardial scar and consequent arrhythmias in ischemic and nonischemic cardiomyopathy. Ebstein’s anomaly may be associated with right sided accessory pathway in ventricular pre-excitation, that is WPW syndrome, with or without atrioventricular re-entrant tachycardia.
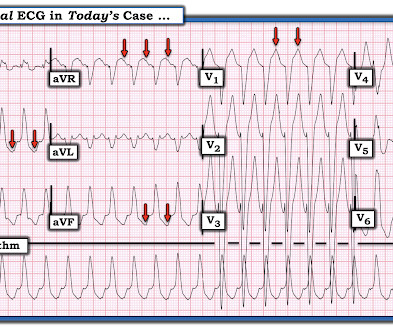
See this even more interesting and more dramatic and fascinating case: History of Hypertrophic Cardiomyopathy (HOCM), with Tachycardia and High Lactate = My Comment by K EN G RAUER, MD ( 10/28 /2023 ): = QUESTION: For clarity in Figure-1 — I've reproduced today's ECG without the long lead rhythm strip. 23/WCC — 2/21/2020 ).
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.








































Let's personalize your content