This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Using ECG recording and deductive reasoning, our teachers and predecessors classified the bradycardias and tachycardias and proposed many mechanisms, subsequently proven to be correct. Notwithstanding many insightful observations, the electrocardiogram (ECG) arguably ignited the big bang in our understanding of cardiac arrhythmias.
Additionally, there was no significant progression of pericardial effusion.DiscussionThe primary strategies for alleviating LVOT obstruction involve altering the structure of the septum, including septal myectomy (SME), alcohol septal ablation (ASA), and septal radiofrequency ablation.
Among athletes with AF, long term medical therapy may be sub-optimal due to baseline bradycardia, potential impact on peak performance, and/or patient preference. AF ablation has evolved as suitable first line therapy for rhythm control and symptom mitigation.
It is mediated by vagal reflexes causing bradycardia or asystole through cardioinhibitory mechanisms. Treatment ranges from lifestyle modifications and pharmacologic interventions to pacemaker implantation or cardioneural ablation.
Cardioneuroablation (CNA) is an emerging therapy for patients with vagally mediated bradycardia/syncope targeting the epicardial ganglionated plexi (GP) surrounding the caval veins and the atria. Only radiofrequency ablation (RFA) has been used to achieve this goal thus far.
Ablation for WPW can be challenging when there is intermittent or weakened accessory pathway conduction. Cardiac effects include bradycardia and AV conduction delay. Neostigmine is an anticholinesterase drug used to antagonize non-depolarizing neuromuscular blocking agents (often in conjunction with glycopyrrolate or atropine).
The authors should be congratulated on their study, concluding that initiating pulsed field ablation (PFA) from the right superior PV (RSPV) could potentially prevent vagal pauses caused by PFA of the left PV antrum, thereby eliminating the necessity for pacing support.
In a case report published in 1984 in the New England Journal of Medicine, Figure 1 was an electrocardiogram that showed sinus bradycardia with a short PR interval and prominent delta waves, with a pattern of preexcitation typical of a posteroseptal accessory pathway (PSAP).1
Chronic recurrent monomorphic VT like fascicular tachycardia and right ventricular outflow tract tachycardia are also amenable to electrophysiological mapping and ablation. Recurrent ventricular tachycardia in spite of radiofrequency catheter ablation needs an implantable cardioverter defibrillator.
Abstract Introduction Severe transitory episodes of bradycardia with subsequent syncope in children are common, and generally portend a benign prognosis. Rarely, patients may experience prolonged asystolic episodes secondary to significant sinus pauses (SP) or paroxysmal atrioventricular block (AVB).
Ablation to prevent recurrent flutter was performed. These include not only induction of significant bradycardia ( albeit usually short-lived ) — but also both ventricular and supraventricular tachyarrhythmias. The subsequent EP study could not induce VT, only atrial fibrillation.
3] So a patient with WPW can have the pattern induced by ischemia, and there is also a report of a patient with pre-existing WPW which was “ablated” by myocardial infarction after an LAD occlusion.[4] Delta waves are seen in 11/12 leads. In most of these leads — the PR interval is clearly shortened, with resultant QRS widening.
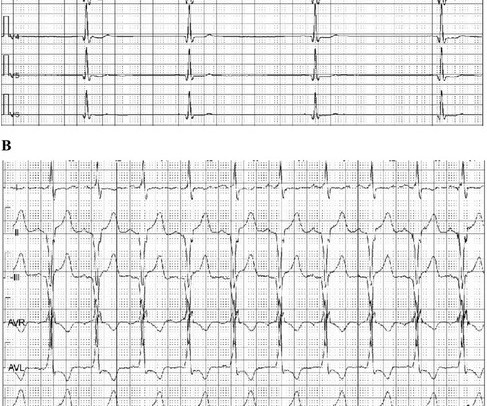
There was no evidence bradycardia leading up to the runs of PMVT ( as tends to occur with Torsades ). If there had been — a temporary atrial pacemaker could have been considered as a way of increasing the heart rate to suppress a bradycardia-dependent arrhythmia ("overdrive pacing").
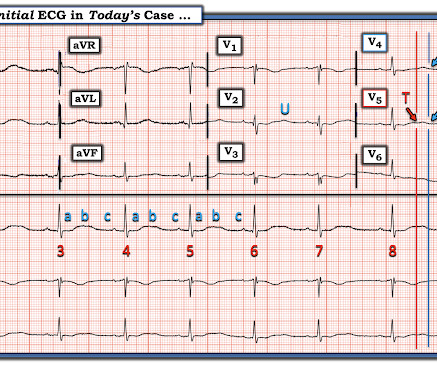
This ECG shows sinus bradycardia with massively long QT (or QU?) Especially when present in the setting of bradycardia and syncopal episodes, this is very worrisome for high risk of lethal dysrhythmias including polymorphic ventricular fibrillation (termed Torsades when in the setting of long QT). interval, at over 600 msec.
Conclusions This study is expected to provide valuable findings regarding arrhythmia in HFnon-rEF patients, and elucidate a potential new therapeutic approach for HFnon-rEF.
Invasive ablation procedure are reserved for a fraction of the population. Any good physician can easily recognize and manage this arrhythmia with simple measures, advices and liberal use of beta blockers, without the need of tricky drugs like Amiodarone.
There are 2 main options: Overdrive pacing could be considered and in the right clinical situation, this is often effective for reducing ventricular arrhythmias ( especially in the case of preventing pause induced or bradycardia-induced arrhythmias in association with QTc prolongation ). Try a different kind of antiarrhythmic.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




















Let's personalize your content