This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Radiofrequency ablation (RFA) is an important therapeutic modality for atrial fibrillation (AF), widely utilized in clinical practice due to its safety and significant efficacy. This case report describes a unique instance of a patient developing AEF following AF ablation, accompanied by ischemic stroke and myocardial infarction.
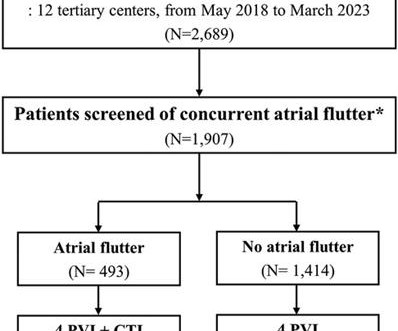
Typical atrialflutter commonly occurs in patients with atrial fibrillation (AF). Limited information exists regarding the effects of concurrent atrialflutter on the long-term outcomes of rhythm control. The data were obtained from a multicenter registry of cryoballoon ablation for AF ( n = 2,689).
Outcomes of ablation with the FARAPULSE PFA System – a nonthermal treatment in which electric fields selectively ablate heart tissue – will be compared to outcomes following use of anti-arrhythmic drug (AAD) therapy, which is commonly prescribed for patients living with persistent AF. The company now anticipates U.S. Circulation.
Idiopathic atypical (non-cavotricupid isthmus [CTI]-dependent) atrialflutter (IAAFL) may be seen in patients without structural heart disease and without previous cardiac surgery or ablation.
Food and Drug Administration (FDA), has granted approval to Boston Scientific for its FARAPULSE Pulsed Field Ablation System. intermittent) atrial fibrillation (AF) and is a unique new alternative to standard-of-care thermal ablation treatment. said Nick Spadea-Anello, president, Electrophysiology, Boston Scientific. "The
ABSTRACT Atrialflutter (AFL), defined as macro-re-entrant atrial tachycardia, is associated with debilitating symptoms, stroke, heart failure, and increased mortality. Atypical AFL is a heterogenous group of re-entrant atrial tachycardias that most commonly occur in patients with prior heart surgery or catheter ablation.
Atypical AtrialFlutter (AAFL) prevalence is increasing due to the escalating Atrial Fibrillation (AF) ablations and cardiac surgeries. We wanted to explore the outcome of the AAFL ablation, considering the recent changes in mapping and ablation.
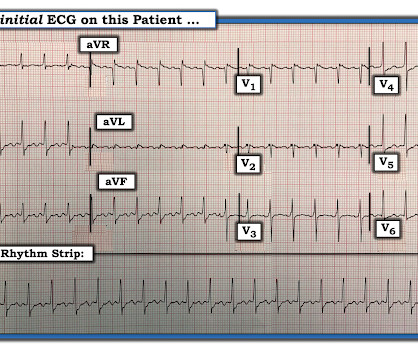
Atrialflutter with 2:1 conduction. The atrialflutter rate is approximately 200 bpm, with 2:1 AV conduction resulting in ventricular rate almost exactly 100 bpm. Further history revealed she had new onset atrialflutter soon after her aortic surgery, and was put on flecainide approximately 1 month ago.
Single-shot pulsed field ablation (PFA) catheters for pulmonary vein isolation are being studied. However, there is a need to deliver flexible lesions for atrialflutter (AFL) and non-PV ablations. A 7Fr PFA catheter (PFLinear, EnChannel Medical) capable of delivering both focal and linear ablations has been developed.
BackgroundTypical isthmus-dependent atrialflutter (AFL) is traditionally treated through radiofrequency (RF) ablation to create a bidirectional conduction block across the cavo-tricuspid isthmus (CTI) in the right atrium.
Cavo-tricuspid isthmus (CTI) dependent atrialflutter (AFL) is one of the most common atrial arrhythmias involving the right atrium (RA). Radiofrequency catheter ablation has been widely used as a therapy of choice and it is curative.
A significant proportion of patients with isolated atrialflutter (AFL) will develop atrial fibrillation (AF) following cavotricuspid isthmus (CTI) ablation.
Abstract Introduction Cavo-tricuspid isthmus (CTI) dependent atrialflutter (AFL) is one of the most common atrial arrhythmias involving the right atrium (RA) for which radiofrequency catheter ablation has been widely used as a therapy of choice. There was a significant reduction in left atrial volume index (82.74 ± 28.5
Image-based patient-specific computational models have recently emerged as a tool to guide atypical atrialflutter (AAF) ablation. However, little is known about the sensitivity of these models to the selection of parameters.
Wild-type transthyretin amyloid cardiomyopathy (ATTRwt-CM) is often accompanied by atrial fibrillation (AF), atrialflutter (AFL), and atrial tachycardia (AT), which are difficult to control because beta-blockers and antiarrhythmic drugs can worsen heart failure (HF).
Pulsed field ablation (PFA) is a non-thermal ablative strategy that achieves cell death via electroporation. Recently, this modality has been utilized for ablation of the cavotricuspid isthmus (CTI) for treatment of atrialflutter.
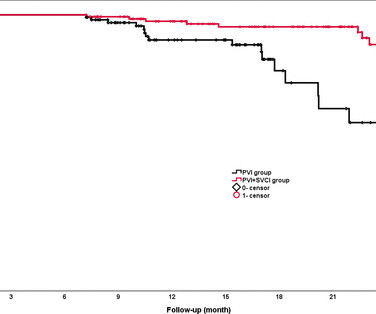
Background The value of empirical superior vena cava isolation (SVCI) following pulmonary vein isolation (PVI) to improve the efficacy of radiofrequency catheter ablation (RFCA) for paroxysmal atrial fibrillation (PAF) remains controversial. RFCA was guided by quantitative AI in both groups. vs 81.5%, p=0.02). 95% CI 0.19
When mutiple atrial tachycardias coexist, ablation of an individual isthmus may lead to a seamless transition (without significant changes in surface ECG or coronary sinus activation) to a second rhythm. The isthmus block could go unnoticed leading to continued unnecessary ablations.
Radiofrequency ablation (RFA) of cavotricuspid isthmus (CTI)dependent atrialflutter requires ablation of the tricuspid annulus overlying the right coronary artery (RCA). Although it is considered safe, reports of acute and subacute RCA injury in human and animal studies raise the possibility of late RCA stenosis.
Atrial fibrillation (AF) is the most common cardiac arrhythmia with increasing prevalence globally. Catheter ablation is well-established treatment for prevention of AF recurrences and decreasing AF symptoms.
Cheng and Zhang to our paper1, we note that despite ARVC being a relatively uncommon cardiomyopathy, we uniquely report on a large clinical experience with very long-term follow-up after VT ablation and confirm a high incidence of atrialflutter (AFL) and the effectiveness and low risk of catheter ablation of AFL.
The positive F wave in lead V1 changed during entrainment from the right atrial appendage (RAA) during typical atrialflutter (AFL). Abstract Introduction Typical atrialflutter (AFL) is a macroreentrant tachycardia in which intracardiac conduction rotates counterclockwise around the tricuspid annulus.
Ablation of isthmus-dependent atrialflutter with interventional CMR has demonstrated its efficacy and safety in the initial phase for achieving bidirectional block. However, limited long-term follow-up data exist for these patients.
Complete and durable block across the left atrial (LA) roof can be integral to ablation of persistent atrial fibrillation (AF) and atypical atrialflutter (AFl). The right pulmonary artery (RPA) is in close proximity to the LA roof, and may provide a vantage for epicardial LA roof mapping and ablation.
Recurrence rates after catheter ablation in these patients are high. Demographic, clinical, and outcome variables over 5 years were compared between patients with and without SVT recurrence.Results:Mean age of 25 patients (56% male) at time of SVT ablation was 31.5 ± 7.2 Ablation success rate was 92%.
FAAM ablation successfully decreased the recurrence rate of atrial tachyarrhythmia compared with conventional non-PV foci ablation. Abstract Introduction Treatment of recurrent atrial fibrillation (AF) is sometimes challenging due to non-pulmonary vein (PV) foci. The RHYTHMIA system was used to perform all the procedures.
BACKGROUND:Inflammation may promote atrial fibrillation (AF) recurrence after catheter ablation. This study aimed to evaluate a short-term anti-inflammatory treatment with colchicine following ablation of AF.METHODS:Patients scheduled for ablation were randomized to receive colchicine 0.6 2.02];P=0.89). 1.99];P=0.55).CONCLUSIONS:Colchicine
Abstract The QDOT MICRO™ Catheter is a novel open-irrigated contact force-sensing radiofrequency ablation catheter. It offers very high-power short-duration (vHPSD) ablation with 90 W for 4 s to improve safety and efficacy of catheter ablation procedures.
Cavotricuspid isthmus (CTI) ablation is crucial to right atrialflutter (AFL) and persistent atrial fibrillation (AF). Identification and eradication of this electric pathway is important to prevent the recurrence of atrial arrhythmias.
To me, it was clearly atrialflutter with 1:1 conduction. The rate of 280 is just right for atrialflutter. The waves look like atrialflutter waves, NOT like a wide ventricular complex. Reverted to atrial fibrillation with RVR while in the hospital 3 times and needed cardioversion.
Publication date: Available online 17 December 2023 Source: The American Journal of Cardiology Author(s): Hugo De Larochellière, François Brouillette, Patrick Lévesque, Nicolas Dognin, Raphaël St-Germain, Goran Rimac, Sylvain Lemay, François Philippon, Mario Sénéchal
67-year-old male has a planned PVI with RFA for atrial fibrillation involving bilateral wide area circumferential ablation, left carina line, posterior left atrial linear box isolation. He also underwent separate CTI ablation for atrialflutter. He was discharged the next day on colchicine and omeprazole.
Pulmonary vein isolation (PVI) remains the cornerstone of atrial fibrillation (AF) ablation. In patients with more advanced AF subtypes, atypical atrialflutter, and extensive atrial myopathy, additional linear ablation is often required; however, durable block of these remains challenging.
In contrast to other tachycardias, with atrial fibrillation (AF), the focus is often speculative, and ablation attempts are made accordingly. Pulmonary veins have been the primary target for ablation for many years, yet the success rates remain inconsistent. We know atrialflutters can be confined to one atrium.
Abstract Introduction Atrial fibrillation and atrialflutter originating from the donor s heart is a commonly reported complication post heart transplant. Electrophysiologic study demonstrated atrial fibrillation originating from native heart and propagated through atrio-atrial connections to the donor heart.
The WCT is interrupted by a series of variable-morphology QRS complexes, with atrialflutter waves note in II, III, and aVF. Detail of Flutter waves The rate of the flutter waves matches the rate of the WCT (about 200/m), proving that the presenting WCT had been 1:1 atrialflutter.
PubMed was queried for entries on AF and rurality: (atrial fibrillation OR atrialflutter) AND (rural OR urban OR rurality OR metro OR metropolitan) AND (united states OR US OR U.S.) The use of catheter ablation for AF per electrophysiologist was similar across the ruralurban spectrum. published up to September 24, 2023.
The ECG was interpreted as showing atrialflutter with 2:1 conduction. The heart rate could be compatible with that of a 2:1 conducted atrialflutter. Also, lead I could give the initial impression of showing flutter waves. After atrial rhythm/SR was restored the patient slowly improved.
Abstract Background Dofetilide is a class III antiarrhythmic agent approved for the treatment of atrial fibrillation and atrialflutter. Prior catheter ablation had been performed in 33 patients (41%). A80% decrease in PVC burden was defined as a satisfactory response. An ICD was present in 72 patients (89%).
PEARL # 3: AtrialFlutter with 1:1 AV conduction is rare! Since the rate of atrial activity with flutter in adults is most often very close to 300 /minute ( ie, usual range for atrial activity ~250-350/minute ) — AFlutter with 2:1 AV conduction typically results in a regular ventricular rate of ~140-160/minute.
The differential of a regular narrow QRS tachycardia is sinus tachycardia, SVT, and atrialflutter with regular conduction. There are no P waves preceding the QRS complexes, and no clear flutter waves. There is no need to immediately refer today’s patient to EP for ablation.
The principal d ifferential d iagnosis i s similar to what we derived in the October 16, 2019 Case : i ) Sinus Tachycardia ; ii ) Reentry SVT ( either A VNRT if the reentry circuit is contained within the normal AV nodal pathway — or A VRT if an accessory pathway is involved ) ; iii ) Atrial Tachycardia ; or iv ) AtrialFlutter.
The Differential Diagnosis is: SVT with aberrancy(#) [AVNRT vs. WPW (also called AVRT*)] Atrialflutter with 1:1 conduction, with aberrancy VT coming from the anterior fascicle ( fascicular VT )@ *AVRT = AV Reciprocating Tachycardia (Tachycardic loop that uses both the AV node and an accessory pathway.
a global leader in cardiac arrhythmia treatment and part of Johnson & Johnson MedTech , today announced European CE mark approval of the VARIPULSE Platform for the treatment of symptomatic drug refractory recurrent paroxysmal atrial fibrillation ( AF ) using pulsed field ablation (PFA).
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.








































Let's personalize your content