This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Outcomes of ablation with the FARAPULSE PFA System – a nonthermal treatment in which electric fields selectively ablate heart tissue – will be compared to outcomes following use of anti-arrhythmic drug (AAD) therapy, which is commonly prescribed for patients living with persistent AF. The company now anticipates U.S. Circulation.
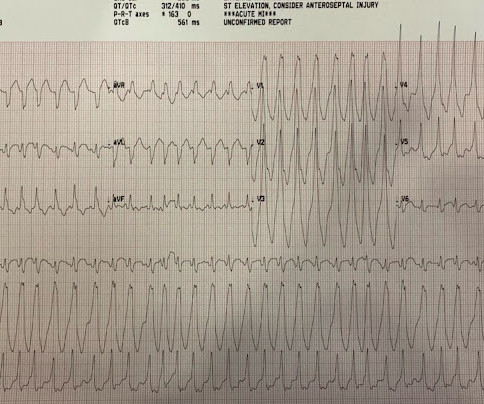
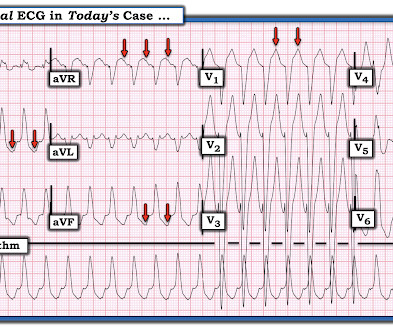
The ECGs show a wide complex, irregularly irregular tachycardia. The differential of wide complex irregularly irregular includes: polymorphic VT, atrialfibrillation with WPW, atrialfibrillation with other aberrancy. Thus, the patients rhythm is atrialfibrillation with WPW.
When atrialfibrillation (AF) begins, it can start with a single focus, degenerating to multiple wavelets, and it spreads throughout the entire surface area of both atria. A fibrillatory wave that occurs at a rate of more than 600 beats per minute can cause fatigue in the long run, leading to atrial dilation.
But it is not disorganized enough to be polymorphic ventricular tachycardia. The rhythm is therefore atrialfibrillation with WPW until proven otherwise. The patient did well and was referred for ablation. Learning Points: Wide complex irregularly irregular tachycardias include PMVT, AF with WPW, and AF with aberrancy.
Abstract Introduction Some previous studies have reported that a first-step ethanol infusion into the vein of Marshall (EIVOM) with touch-up radiofrequency (RF) ablation can facilitate mitral isthmus (MI) block and improves the ablation outcomes in persistent atrialfibrillation (PeAF) patients. 0.78, p = .006).
Atrioventricular junction ablation (AVJA) is used as an alternative treatment for patients with atrialfibrillation (AF) to regularize ventricular rates with pacing. Although a reduction in atrialtachycardia/atrialfibrillation (AT/AF) burden in these patients has been reported, its incidence remains unknown.
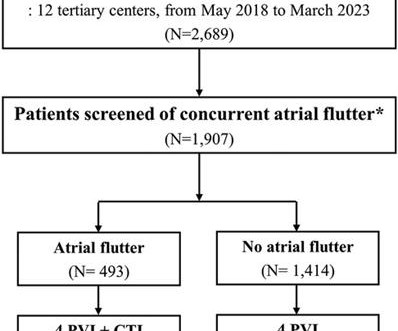
Typical atrial flutter commonly occurs in patients with atrialfibrillation (AF). Limited information exists regarding the effects of concurrent atrial flutter on the long-term outcomes of rhythm control. The data were obtained from a multicenter registry of cryoballoon ablation for AF ( n = 2,689).
Catheter ablation of atrialfibrillation (AF) has become a standard of care for symptomatic patients. However, atrialtachycardias (ATs) may develop in a portion of such patients, and mapping and ablating these can be challenging.
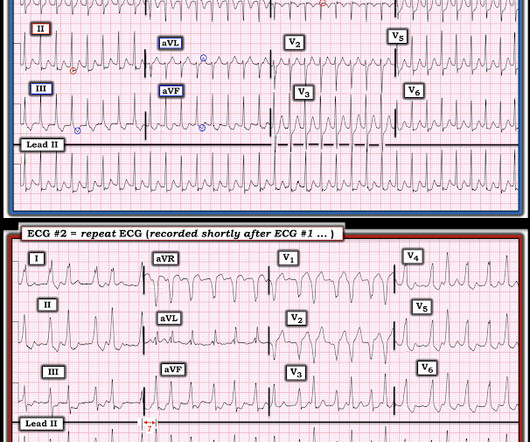
A prehospital 12-lead was recorded: There is a regular wide complex tachycardia. The computer diagnosed this as Ventricular Tachycardia. There is a wide complex regular tachycardia at a rate of 226. Toothache, incidental Wide Complex Tachycardia Could it be fascicular VT or Bundle Branch VT ( i.e., idiopathic VT )?
The two ECGs above were texted to me with the text: "Young Guy came in in SVT but now in and out of irregular wide complex tachycardia. -- not sure if polymorphic VT vs. a fib with WPW." Definitely atrialfibrillation. Probably WPW but is very slow for atrial fib withWPW. So this looks like WPW with Atrialfibrillation.
Biatrial atrialtachycardia (BiAT) is a rare form of atypical macro-reentrant AT (MRAT) that can be difficult to characterize and ablate. Ablation of regions demonstrating spatiotemporal dispersion (SD) has shown a high rate of atrialfibrillation (AF) termination to either sinus or MRAT during ablation.
Epicardial Marshall bundle (MB) are frequently utilized in left atrialtachycardias (LATs) post atrialfibrillation (AF) ablation with pulmonary vein isolation and substrate modification.
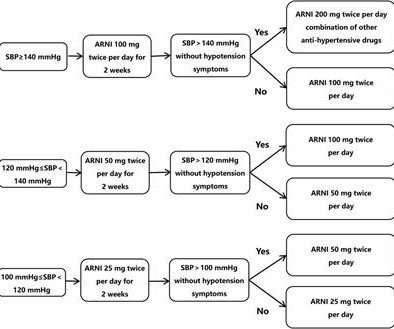
Introduction A high recurrence rate of atrialfibrillation was monitored after catheter ablation for persistent atrialfibrillation. The results will evaluate sacubitril/valsartan as a novel treatment for improving prognosis and a complement to conventional drug therapy.
Ablation of regions demonstrating spatiotemporal dispersion (SD) has been demonstrated as an alternative strategy beyond pulmonary vein isolation in patients with persistent atrialfibrillation. Occurrence of atrialtachycardia (AT) following ablation remains a limitation of this approach.
Vein of Marshall ethanol ablation (VOM-EA) as an adjunct to pulmonary vein isolation (PVI) has been reported to improve freedom from atrialfibrillation (AF) and atrialtachycardia (AT).
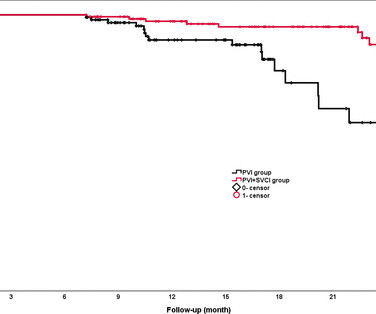
Background The value of empirical superior vena cava isolation (SVCI) following pulmonary vein isolation (PVI) to improve the efficacy of radiofrequency catheter ablation (RFCA) for paroxysmal atrialfibrillation (PAF) remains controversial. RFCA was guided by quantitative AI in both groups. vs 81.5%, p=0.02). 95% CI 0.19
Backgroundwide antral pulmonary vein isolation (PVI) is effective for treating paroxysmal atrialfibrillation (PAF), although time-demanding. Procedural data and electrophysiology (EP) laboratory times were systematically collected and analyzed.
Contemporary pulse field ablation (PFA) systems have been developed for the treatment of atrialfibrillation, but the unique biophysical properties of PFA may provide advantages for the treatment of ventricular tachycardia (VT).
The Kaplan-Meier curve of all-atrial arrhythmia-free survival for (A) all persistent patients and (B) patients who underwent PSM conducted to the higher recurrence rate in PVI + group. At 1-year follow-up, the PVI only group showed significantly fewer atrial tachyarrhythmia recurrences compared to PVI + group (69% vs. 56%, p =0.013).
A patient in the ICU with significant underlying cardiac disease [HFrEF 30%, non-ischemic cardiomyopathy, LBBB s/p CRT-D (biventricular pacer), AVNRT s/p ablation a few yrs ago, hx sinus tachycardia while on max tolerated BB therapy] went into a regular wide-complex tachycardia after intubation for severe COPD exacerbation.
Vein of Marshall ethanol ablation (VOM-EA) as an adjunct to pulmonary vein isolation (PVI) has been reported to improve freedom from atrialfibrillation (AF) and atrialtachycardia (AT).
She also has a hx of paroxysmal atrialfibrillation and is on oral anticoagulant treatment. She had a single chamber ICD/Pacemaker implanted several years prior due to ventricular tachycardia. Answer : The ECG above shows a regular wide complex tachycardia. Cardiac output (CO) was being maintained by the tachycardia.
The AWARE-RCT (JAMA Cardiology 2023) evaluated the efficacy of an augmented ablation strategy involving a second, wide area circumferential catheter ablation (double WACA) compared to the standard arm (single WACA) in patients with paroxysmal atrialfibrillation (AF).
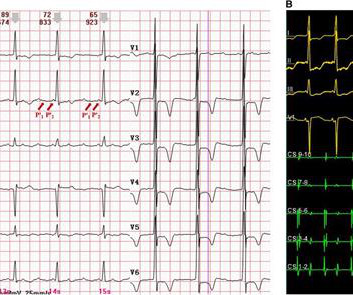
However, widely split P' waves in focal atrialtachycardia (AT) on a surface electrocardiogram (ECG) have rarely been reported. Case summary A 67-year-old patient, who had undergone two radiofrequency ablations for atrialfibrillation, presented with recurrent palpitation.
Wild-type transthyretin amyloid cardiomyopathy (ATTRwt-CM) is often accompanied by atrialfibrillation (AF), atrial flutter (AFL), and atrialtachycardia (AT), which are difficult to control because beta-blockers and antiarrhythmic drugs can worsen heart failure (HF).
Whenever it is this fast, you need to be very careful to ascertain whether it is irregular ( as in atrialfibrillation with rapid ventricular respsonse ) or regular ( as in VT ). This is not because it is polymorphic VT; it is because it is WPW with atrialfibrillation. A anterolateral AP was successfully ablated.
Spatiotemporal electrogram dispersion areas (STED) have been proposed as promising targets for substrate/driver ablation in persistent atrialfibrillation (PsAF).
Pulse field ablation (PFA) using a pentaspline catheter is an effective and safe treatment method for pulmonary vein isolation (PVI) in patients with atrialfibrillation (AF).1,2 We present a case of a macro-reentrant atrialtachycardia in the lateral right atrium (RA) treated by PFA using a pentaspline catheter.
Radiofrequency catheter ablation (RFCA) for persistent atrialfibrillation (AF) is associated with suboptimal long-term outcomes. Although increasing evidence supports substrate-based ablation strategies targeting extra-PV sources, reliable endpoints during CA beyond pulmonary vein (PV) isolation are not well established.
Commonly employed empiric strategies for catheter ablation (CA) of refractory atrialfibrillation (AF) beyond pulmonary vein isolation (PVI) include posterior wall isolation (PWI), linear ablation involving left atrial (LA) roof and mitral lines, as well as targeting of areas of low voltage / myopathy.
Abstract Introduction Atrialfibrillation and atrial flutter originating from the donor s heart is a commonly reported complication post heart transplant. Case A 47-year-old male presented with atrialtachycardia 6 months post heart transplant.
BACKGROUND:Inflammation may promote atrialfibrillation (AF) recurrence after catheter ablation. This study aimed to evaluate a short-term anti-inflammatory treatment with colchicine following ablation of AF.METHODS:Patients scheduled for ablation were randomized to receive colchicine 0.6 2.02];P=0.89).
1 Thereafter, its indications broadened to include neurolysis, myocardial septal ablation in hypertrophic cardiomyopathy,1 and, most recently as an off-label use, retrograde venous infusion for ablation of cardiac arrhythmias such as atrialfibrillation (AF), ventricular tachycardia (VT), and premature ventricular complexes (PVCs).2
FAAM ablation successfully decreased the recurrence rate of atrial tachyarrhythmia compared with conventional non-PV foci ablation. Abstract Introduction Treatment of recurrent atrialfibrillation (AF) is sometimes challenging due to non-pulmonary vein (PV) foci.
Patients with congenital heart disease (CHD) are at high risk for supraventricular tachyarrhythmias including atrialfibrillation (AF) and atrialtachycardia (AT).
Pulsed field ablation (PFA) is a reliable treatment modality in the pulmonary vein (PV) antra and the left atrial posterior wall (LAPW), but lesion durability in other atrial segments may be less optimal with the current PFA systems.
Pulsed field ablation (PFA)-induced electroporation is an application of high-energy, direct-current shocks on myocardium albeit at a considerably lower current density that decreases the risks of arcing and barotrauma.1
Pulsed field ablation (PFA) is a non-thermal ablation technology, utilising the mechanism of electroporation to interrupt the cellular membrane and induce myocyte apoptosis.
Abstract Introduction Despite advanced ablation strategies and major technological improvements, treatment of persistent atrialfibrillation (AF) remains challenging and the underlying pathophysiology is not fully understood. ms after) and AF termination to atrialtachycardia (AT) or sinus rhythm (SR) in 12 patients (24%).
15% of all atrialfibrillation (AF) patients who undergo catheter ablation and plays significant roles in arrhythmia recurrence.1,2 1,2 Eliminating identified extra-PV triggers is an important part of an AF ablation procedure after pulmonary vein isolation (PVI) is achieved.3
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.







































Let's personalize your content