This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
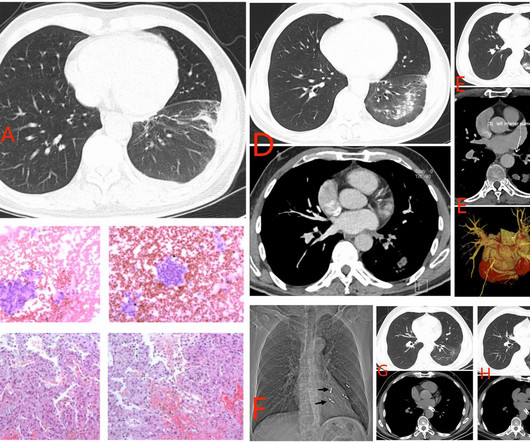
The increased use of radiofrequency ablation (RFA) for atrialfibrillation (AF) has led to a rise in cases of pulmonary vein stenosis or occlusion (PVS/O) as a complication. The actual frequency of pulmonary vein (PV) occlusion remains a topic of debate.
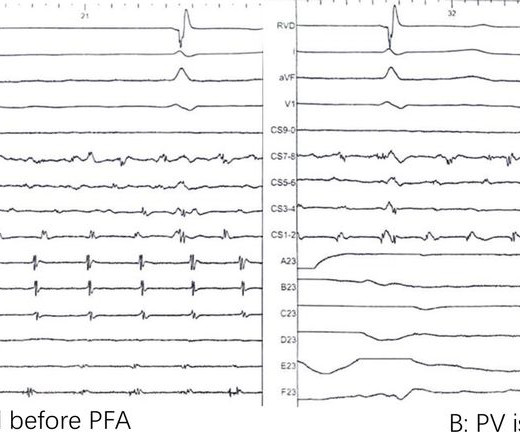
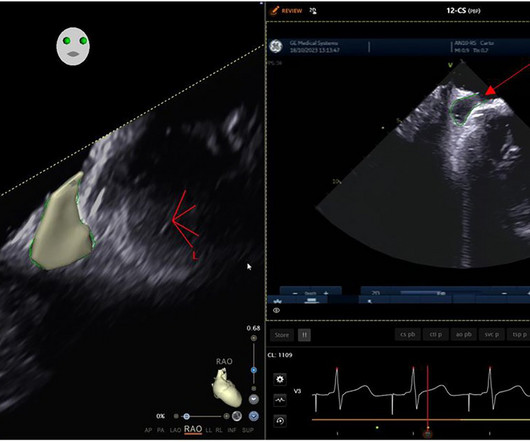
Objective Pulsed-field ablation (PFA) is a new technology of catheter ablation for atrialfibrillation (AF). This research is to investigate the feasibility of a new strategy (transoesophageal echocardiography-guided pulsed field ablation, TEEP) to guide PFA for AF with no contrast and zero fluoroscopy.
Atrialfibrillation is the most prevalent arrhythmia with a lifetime risk of nearly 30%. Pulmonary vein isolation (PVI) is the most effective treatment for rhythm control. It can be associated with reduced quality of life and complications such as heart failure and stroke.
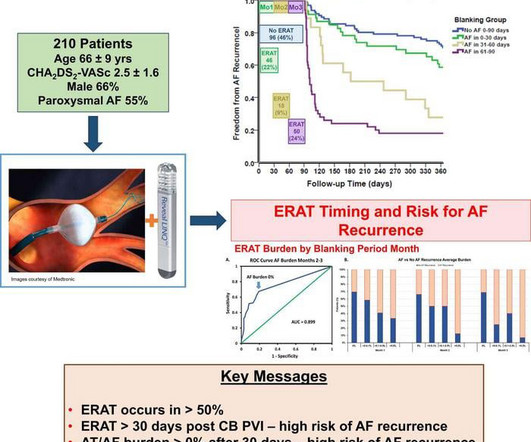
Based on continuous monitoring of early recurrence of atrial tachyarrhythmia immediately after patients have undergone atrialfibrillationablation, Musat et al. ERAT is often attributed to transient inflammation induced by tissue damage during ablation and short-term imbalances in autonomic innervation.
Outcomes of ablation with the FARAPULSE PFA System – a nonthermal treatment in which electric fields selectively ablate heart tissue – will be compared to outcomes following use of anti-arrhythmic drug (AAD) therapy, which is commonly prescribed for patients living with persistent AF. The company now anticipates U.S. Circulation.
Focal coronary spasm is a recognised complication of pulsed field ablation (PFA) delivered within proximity of coronary arteries (1). There have been 2 recent case reports of focal spasm occurring during pulmonary vein isolation (PVI) for atrialfibrillation (AF) using PFA remote from coronary arteries (2,3).
Ablation index (AI)-guided pulmonary vein isolation (PVI) has enhanced procedural outcomes for atrialfibrillation (AF).1 1 However, patients with persistent AF present higher recurrence rates due to advanced atrial remodeling,2-3 represented by the left atrial low voltage area (LVA), compared to those with paroxysmal AF.
ABSTRACT Introduction Pulsed Field Cryoablation (PFCA) is a dual-energy cardiac ablation modality consisting of short-duration ultra-low temperature cryoablation (ULTC) followed immediately by pulsed field ablation (PFA) delivered from the same catheter. Results Sixty-six patients were ablated at six sites.
Pulsed field ablation (PFA) for paroxysmal atrialfibrillation (AF) has been gaining worldwide acceptance due to its efficacy and safety. However, the role of TPI during pulmonary vein (PV) isolation (PVI) is unclear. A variable loop circular catheter (VLCC, VARIPULSE, Biosense Webster, Inc.)
Research conducted across 12 hospitals in China has discovered that combining linear ablation with ethanol infusion via the vein of Marshall (EIVOM) alongside pulmonary vein isolation (PVI) significantly improves sinus rhythm maintenance in patients suffering from persistent atrialfibrillation.
Pulmonary vein isolation (PVI) is the cornerstone of interventional treatment for atrialfibrillation (AF). Pulsed-field ablation (PFA), a novel non-thermal modality, was recently introduced and is now available with four different FDA-approved systems from three different manufacturers.
Expanding the potential patient population for pulsed field ablation, results from the SINGLE SHOT CHAMPION study suggest PFA might be just as good as cryoballoon ablation for patients with paroxysmal AFib. PFA has shown advantages in procedure time and safety, but its effectiveness is unproven compared to cryoballoon ablation.
(MedPage Today) -- LONDON -- Pulmonary vein isolation (PVI) produced real short-term improvements for people with atrialfibrillation (Afib or AF), according to the first sham-controlled trial on the subject. Continuous monitoring by implantable.
The international, multi-center trial will provide clinical evaluation of Cortex's 510(k) cleared Ablamap System with electrographic flow (EGF) and newly released Ablacath Mapping Catheter basket mapping catheter to identify extra-pulmonary vein EGF sources. and may enroll up to 400 subjects across 20+ centers in the US and Europe.
(MedPage Today) -- The FDA approved the Farapulse pulsed field ablation (PFA) system for paroxysmal atrialfibrillation (Afib or AF), Boston Scientific announced on Wednesday. The device won an indication for the isolation of pulmonary veins in.
Both atria develop from a combination of the primitive atrium, sinus venous, and pulmonary veins.It When atrialfibrillation (AF) begins, it can start with a single focus, degenerating to multiple wavelets, and it spreads throughout the entire surface area of both atria. The baseline RA dimension is a few mm more than LA.
Food and Drug Administration (FDA), has granted approval to Boston Scientific for its FARAPULSE Pulsed Field Ablation System. A company statement reported that its PFA System is indicated for the isolation of pulmonary veins in the treatment of drug-refractory, recurrent, symptomatic, paroxysmal (i.e.,
Initial findings from feasibility studies on pulsed field ablation (PFA) in the treatment of atrialfibrillation (AF) indicated high rates of efficacy and pulmonary vein (PV) isolation (PVI) durability upon systematic remapping.
a medical device company dedicated to advancing ablation treatment for cardiac arrythmias, announced its participation at the Heart Rhythm 2024 conference, taking place in person at the Boston Convention & Exhibition Center and virtually, May 16-19, 2024. milla1cf Wed, 05/15/2024 - 19:05 May 15, 2024 — CardioFocus, Inc. ,
Titled "Real-world Data Affirms Safety and Effectiveness of Low/Zero Fluoroscopy AtrialFibrillationAblation," the study was presented as a late-breaker at the 29th Annual International AF Symposium. This is the most commonly used ablation catheter in the world for RF ablation and is fully integrated with the CARTO 3 System.
Abstract Introduction Some previous studies have reported that a first-step ethanol infusion into the vein of Marshall (EIVOM) with touch-up radiofrequency (RF) ablation can facilitate mitral isthmus (MI) block and improves the ablation outcomes in persistent atrialfibrillation (PeAF) patients. 0.78, p = .006).
BackgroundCatheter ablation is frequently used to manage recurrent atrialfibrillation (AF) resistant to drug therapy, with pulmonary vein isolation (PVI) as a key tactic.
Background Pulmonary vein isolation with wide antral ablation leads to better clinical outcomes for the treatment of atrialfibrillation, but the isolation lesion is invisible in conventional cryoballoon ablation. The rate of 12-month freedom from clinical atrial arrhythmia recurrence was 85.1%
Despite the relative efficacy of ablation, the risk of AF recurrence is substantial, particularly in patients with persistent AF (perAF). At present we do not have any reliable intra-procedural electrophysiologic predictors of long-term success of AF ablation other than pulmonary vein isolation.
Objectives This study aimed at exploring how using different kinds of sheaths will affect the very first ablation procedure of apprentices. Methods 15 patients with paroxysmal atrialfibrillation were randomized to used fixed-curve, conventional steerable or visualized steerable sheath, and received complete isolation of pulmonary veins.
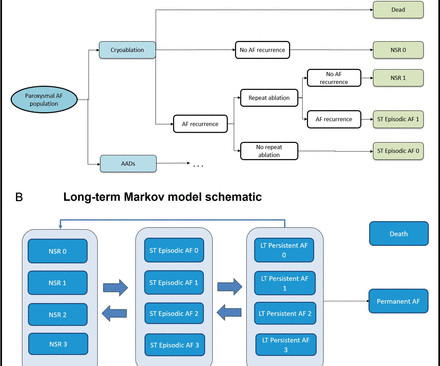
Introduction Three recent randomised controlled trials have demonstrated that pulmonary vein isolation as an initial rhythm control strategy with cryoablation reduces atrial arrhythmia recurrence in patients with symptomatic paroxysmal atrialfibrillation (PAF) compared with antiarrhythmic drug (AAD) therapy.
Background Catheter ablation (CA) for symptomatic atrialfibrillation (AF) offers the best outcomes for patients. We present real-world 5-year follow-up data of AI-guided pulmonary vein isolation. We present real-world 5-year follow-up data of AI-guided pulmonary vein isolation.
Background: Patients with atrialfibrillation (AF) and concomitant pulmonary hypertension (pHTN) have an increased risk of morbidity and mortality. However, the outcomes of catheter ablation in this cohort are unclear.
While atrialfibrillation (AF) ablation has advanced to improve safety, success rates have been slower to improve. Factors contributing to this include the failure to personalize ablation strategies for individuals.
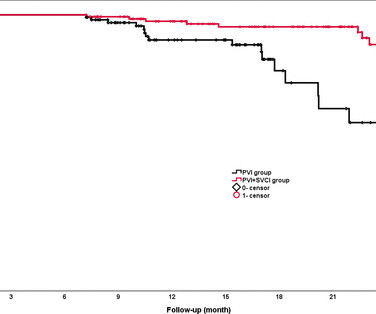
Background The value of empirical superior vena cava isolation (SVCI) following pulmonary vein isolation (PVI) to improve the efficacy of radiofrequency catheter ablation (RFCA) for paroxysmal atrialfibrillation (PAF) remains controversial. RFCA was guided by quantitative AI in both groups. vs 81.5%, p=0.02).
Pulmonary vein (PV) isolation is the cornerstone of radiofrequency (RF) ablation for atrialfibrillation (AF). PV reconnection is the most common cause of recurrent AF following an ablation procedure.
Patients with atrialfibrillation (AF) who undergo repeat ablation are more likely to have non pulmonary vein triggers (NPVTs) identified. The influence of these triggers on future recurrence is yet unknown.
Patients with persistent atrialfibrillation (PeAF) may need additional ablation approaches on the basis of circumferential pulmonary vein isolation (PVI) to maintain long-term sinus rhythm. However, whether ablation of DZs in addition of PVI is effective in PeAF is unknown.
Backgroundwide antral pulmonary vein isolation (PVI) is effective for treating paroxysmal atrialfibrillation (PAF), although time-demanding. Procedural data and electrophysiology (EP) laboratory times were systematically collected and analyzed.
While pulmonary vein isolation (PVI) is a key endpoint for atrialfibrillation (AF) ablation, effective strategies for repeat ablation are debated, particularly when PVs are already isolated.
Pulsed field ablation (PFA) is a novel, nonthermal, cardiac tissue selective ablation modality. To date, radio-frequency (RF) guided high-power-short-duration (HPSD) ablation represents the gold standard for pulmonary vein isolation (PVI) in patients with atrialfibrillation (AF).
Pulmonary vein reconnections (PVRs) remain a concern in atrialfibrillation (AF) ablation. However, the significance of PVR in AF recurrence may differ between patients who undergo additional ablation and those who do not. Eliminating PVRs during redo sessions can lead to favorable rhythm outcomes.
There are limited effective treatment options for persistent atrialfibrillation (AF) ablation. An epicardial-endocardial approach, combining surgical and catheter convergent radiofrequency (RF) ablation, has shown improved outcomes than an endocardial-only RF strategy.
No data have been reported on cooling characteristics and the impact of variant pulmonary vein (PV) anatomy on atrialfibrillation (AF) recurrences after POLARx cryoballoon (CB) ablation.
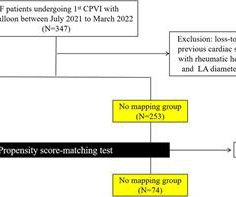
The Kaplan-Meier curve of all-atrial arrhythmia-free survival for (A) all persistent patients and (B) patients who underwent PSM conducted to the higher recurrence rate in PVI + group. At 1-year follow-up, the PVI only group showed significantly fewer atrial tachyarrhythmia recurrences compared to PVI + group (69% vs. 56%, p =0.013).
The Efficacy of Delayed Enhancement MRI-Guided Fibrosis Ablation vs Conventional Catheter Ablation of AtrialFibrillation randomized trial showed no difference in atrialfibrillation (AF) recurrence with additional delayed enhancement magnetic resonance imaging (DE-MRI) fibrosis-targeted ablation to pulmonary vein isolation (PVI) in persistent AF.
Patients undergoing atrialfibrillation (AFib) ablation who were not properly anticoagulated and did not undergo preprocedural transesophageal echocardiogram (TEE) were significantly more likely to suffer from transient ischemic attack (TIA) or pulmonary embolism (PE).
The AFib pulsed field ablation treatment era officially began in the US last week, following the FDA approval of Medtronic’s PulseSelect Pulsed Field Ablation System for the treatment of both paroxysmal and persistent atrialfibrillation.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




































Let's personalize your content