This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
UC San Diego Health is the first in San Diego to successfully implant the world’s first dual chamber and leadless pacemaker system to help treat people with abnormal heart rhythms. Holding the device and pictured above is Ulrika Birgersdotter-Green, MD, cardiologist and director of pacemaker and ICD services at UC San Diego Health.
ABSTRACT Introduction Atrialfibrillation (AF) is the most common arrhythmia, and atrioventricular (AV) node ablation with pacemaker implantation is a therapeutic option for refractory cases. However, AV node ablation in patients with bioprosthetic tricuspid valves poses technical challenges.
16, 2025 Primary results from the DEFINE AFib clinical study show the Medtronic LINQ family of insertable cardiac monitors (ICM), paired with a novel algorithm, were able to detect atrialfibrillation episodes and properly risk stratify patients as high risk prior to an AF-related healthcare utilization 80% of the time. 2024, May 15).
Atrioventricular junction (AVJ) ablation is reserved for patients with refractory uncontrolled atrialfibrillation despite antiarrhythmic drug use or ablation. Atrial lead implant is uncommon during pacemaker implant at the time of AVJ ablation.
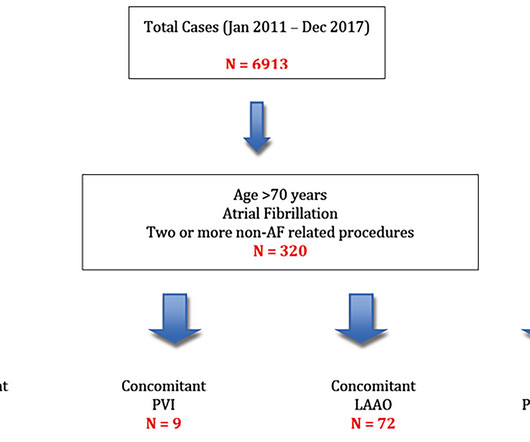
Mehods We retrospectively identified patients aged over 70 years with AtrialFibrillation (AF) from 2011 to 2017 who had two or more other cardiac procedures. Cox-Maze IV AF ablation. No differences observed in freedom from stroke (p = 0.80) or permanent pacemaker (p = 0.33) between the groups.
Abstract Introduction Catheter ablation of atrialfibrillation (AF) has emerged as the most effective therapy. However, rare anatomical abnormalities such as situs inversus totalis, dextrocardia, or interrupted inferior vena cava can make ablation challenging.
Atrioventricular nodal (AVN) ablation with permanent pacemaker implantation – ‘pace and ablate’ – may be considered for patients with symptomatic atrialfibrillation (AF) for whom rhythm control has been unsuccessful. AVN ablation was successful with durable lesions at one year.
AF, atrialfibrillation; ICD, implantable cardioverter defibrillator; ILR, implantable loop recorder. vs. 15.8%; p =0.001), pacemaker implantation (11.2% vs. 1.3%; p =0.996) or catheter ablation (3.8% ABSTRACT Introduction Little is known about age and clinical intervention after implantable loop recorder (ILR) insertion.
The aim of this study is to investigate the usefulness of an implantable loop recorder (ILR) for arrhythmia detection including atrialfibrillation (AF) in HFnon-rEF patients after discharge. Methods and analysis This is a multicentre single arm study to evaluate the usefulness of ILR for detecting arrhythmia.
Abstract Background Cardioneuroablation (CNA) is a novel therapeutic approach for functional bradyarrhythmias, specifically neurocardiogenic syncope or atrialfibrillation, achieved through endocardial radiofrequency catheter ablation of vagal innervation, obviating the need for pacemaker implantation.
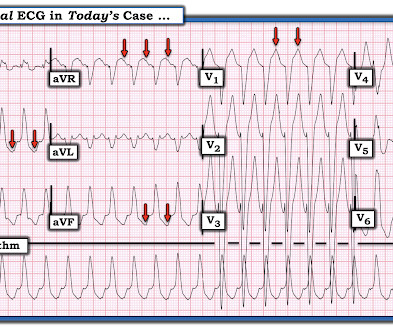
A patient in the ICU with significant underlying cardiac disease [HFrEF 30%, non-ischemic cardiomyopathy, LBBB s/p CRT-D (biventricular pacer), AVNRT s/p ablation a few yrs ago, hx sinus tachycardia while on max tolerated BB therapy] went into a regular wide-complex tachycardia after intubation for severe COPD exacerbation. What to do?
She also has a hx of paroxysmal atrialfibrillation and is on oral anticoagulant treatment. She had a single chamber ICD/Pacemaker implanted several years prior due to ventricular tachycardia. Medical treatment for heart failure was optimized and after a few days the patient was discharged with referral to VT ablation procedure.
ABSTRACT Background Catheter ablation (CA) for atrialfibrillation (AF) in the elderly poses a growing challenge. undergoing index ablation ( n =172/301, 57.1% [PVI only n =156/172, radiofrequency n =92, cryoballoon n =59, pulsed-field ablation n =5]) and re-ablation ( n =129/301 [42.9%]) were included.
The accessory pathway was not further stratified due to evidence of intermittent conduction with a sinus node heart rate of 60bpm, and a bicameral pacemaker was implanted.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

















Let's personalize your content