This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
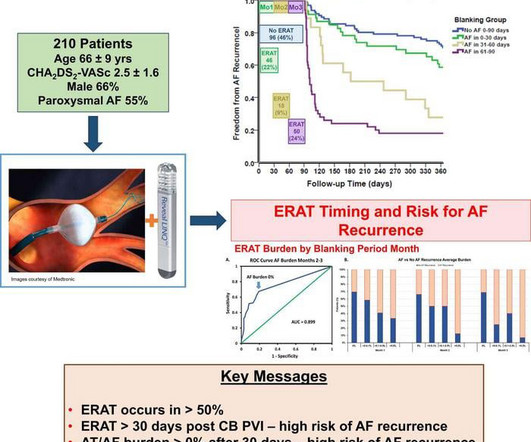
Based on continuous monitoring of early recurrence of atrial tachyarrhythmia immediately after patients have undergone atrial fibrillation ablation, Musat et al. Early recurrence of atrial tachyarrhythmia (ERAT) is commonly seen following catheter ablation of AF, with reported incidences of up to 61% in the first three months.
Atrial fibrillation is the most prevalent arrhythmia with a lifetime risk of nearly 30%. Pulmonary vein isolation (PVI) is the most effective treatment for rhythm control. It can be associated with reduced quality of life and complications such as heart failure and stroke.
Distribution Variance of Focal Atrial Tachycardia Foci and Long-Term Outcomes After Ablation. We aimed to evaluate age differences in foci and factors influencing recurrence after radiofrequency catheter ablation in adult and juvenile patients with FAT. After a mean follow-up of 47.2 months, FAT recurred in 57 patients.
Outcomes of ablation with the FARAPULSE PFA System – a nonthermal treatment in which electric fields selectively ablate heart tissue – will be compared to outcomes following use of anti-arrhythmic drug (AAD) therapy, which is commonly prescribed for patients living with persistent AF. The company now anticipates U.S.
Despite the relative efficacy of ablation, the risk of AF recurrence is substantial, particularly in patients with persistent AF (perAF). At present we do not have any reliable intra-procedural electrophysiologic predictors of long-term success of AF ablation other than pulmonary vein isolation.
a global leader in cardiac arrhythmia treatment and part of Johnson & Johnson MedTechi , revealed findings from a company-funded study of real-world data. Biosense Webster's zero fluoroscopy workflow is the first and only such workflow available in a radiofrequency (RF) cardiac ablation device.
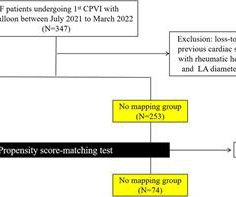
Background Pulmonary vein isolation with wide antral ablation leads to better clinical outcomes for the treatment of atrial fibrillation, but the isolation lesion is invisible in conventional cryoballoon ablation. The rate of 12-month freedom from clinical atrial arrhythmia recurrence was 85.1% min vs. 23.76 ± 8.36 min,
The results of pulmonary vein isolation are limited by arrhythmia recurrence, which is most often due to a failure to effectuate a durable contiguous circumferential transmural lesion around the pulmonary vein (PV) ostia.
Background Catheter ablation (CA) for symptomatic atrial fibrillation (AF) offers the best outcomes for patients. Despite the benefits of CA, a significant proportion of patients suffer a recurrence; hence, there is scope to potentially improve outcomes through technical innovations such as ablation index (AI) guidance during AF ablation.
Patients with D-transposition of the great arteries (D-TGA) palliated with atrial switch often develop atrial arrhythmias (AA) requiring pulmonary venous atrium (PVA) access for ablation, which can be achieved via retrograde aortic approach (RAA) or trans-baffle access (TBA).13
Pulsed field ablation (PFA) may overcome the disadvantages of thermal energy and improve both ablation efficacy and safety. Objective We report the feasibility, safety, and clinical efficacy of focal monopolar PFA in patients with the origin of their atrial arrhythmia in the SVC.
Overview of the study population and effects observed after catheter ablation for atrial fibrillation. PVI, pulmonary vein isolation. Herein we describe the effects of catheter ablation on AF burden, arrhythmia recurrences, and ventricular function in end-stage HF. to 39.18.3% ( p <0.001) following ablation.
Despite advances, catheter ablation success rates for persistent AF remain at 50-60%. The approach for recurrent persistent AF, beyond pulmonary vein isolation, remains contentious. Surgical maze procedures have demonstrated superior outcomes compared to catheter ablation.
ABSTRACT Background Ultra-low temperature cryoablation (ULTC) is a technique designed to rapidly cool cardiac tissue to extremely low temperatures, enabling the creation of ablation lesions for the treatment of atrial fibrillation (AF). Arrhythmia outcomes after repeat ablation were evaluated.
Abstract Background The newly introduced nonthermal pulsed field ablation (PFA) is a promising technology to achieve fast pulmonary vein isolation (PVI) with high acute success rates and good safety features. Data comparing PFA to VHPSD-PVI is lacking. For PFA-PVI a pentaspline 20 electrode catheter was used.
Abstract The QDOT MICRO™ Catheter is a novel open-irrigated contact force-sensing radiofrequency ablation catheter. It offers very high-power short-duration (vHPSD) ablation with 90 W for 4 s to improve safety and efficacy of catheter ablation procedures.
Pulsed Field Ablation is a relatively new modality for treatment of atrial fibrillation. In conventional ablation for atrial fibrillation, either heating of tissue is produced by radiofrequency application or freezing of tissues by cryoablation. Pulsed field ablation group had 305 patients while thermal ablation group had 302 patients.
Circulation: Arrhythmia and Electrophysiology, Ahead of Print. We investigate whether additional linear ablation from the superior vena cava to the right atrial septum and cavotricuspid isthmus ablation improves the rhythm outcome of patients with persistent AF undergoing cryoballoon PVI (Cryo-PVI).METHODS:In
Circulation: Arrhythmia and Electrophysiology, Ahead of Print. BACKGROUND:High-power short-duration ablation has shown impressive efficacy and safety for pulmonary vein isolation (PVI); however, initial efficacy results with very high power short-duration ablation were discouraging. No complications occurred.
Backgroundwide antral pulmonary vein isolation (PVI) is effective for treating paroxysmal atrial fibrillation (PAF), although time-demanding. Procedural data and electrophysiology (EP) laboratory times were systematically collected and analyzed.
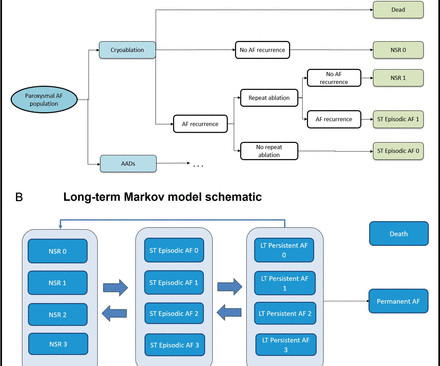
Introduction Three recent randomised controlled trials have demonstrated that pulmonary vein isolation as an initial rhythm control strategy with cryoablation reduces atrial arrhythmia recurrence in patients with symptomatic paroxysmal atrial fibrillation (PAF) compared with antiarrhythmic drug (AAD) therapy. ablations over a lifetime.
Animal studies suggest that catheter ablation-associated parasympathetic and sympathetic denervation could result in increased ventricular arrhythmias (VA). The impact of catheter ablation of atrial fibrillation on VA burden in humans has not been assessed.
Extra-pulmonary vein (PV) triggers have been reported in up to 4.9-15% 15% of all atrial fibrillation (AF) patients who undergo catheter ablation and plays significant roles in arrhythmia recurrence.1,2 Extra-pulmonary vein (PV) triggers have been reported in up to 4.9-15%
Pulsed field ablation (PFA) is a nonthermal energy source for ablation of cardiac arrhythmias. This study investigated the prospective outcomes of a novel PFA generator in conjunction with a commercially available, contact force-sensing, focal ablation catheter.
Both atria develop from a combination of the primitive atrium, sinus venous, and pulmonary veins.It Spatial relationship of sites for atrial fibrillation drivers and atrial tachycardia in patients with both arrhythmias July 2017 International Journal of Cardiology 248(3) AF begets AF. Let us see few factors.
The Kaplan-Meier curve of all-atrial arrhythmia-free survival for (A) all persistent patients and (B) patients who underwent PSM conducted to the higher recurrence rate in PVI + group. Conclusions PVI plus extra PV ablation using a pentaspline PFA catheter is associated with a higher incidence of atrial tachycardia recurrences.
Pulsed field ablation (PFA) has become increasingly important in the treatment of cardiac arrhythmias. In addition to single-shot devices mainly used for pulmonary vein isolation, focal PFA may provide a treatment option that increases the versatility of the technique.
Circulation: Arrhythmia and Electrophysiology, Ahead of Print. Patients were randomly assigned to either the PVI+SVC ablation group or the PVI-only group. CONCLUSIONS:The addition of SVC ablation to PVI did not enhance freedom from atrial tachyarrhythmia at 12 months, and it led to increased complications. versus 72%;P=0.41).
Circulation: Arrhythmia and Electrophysiology, Ahead of Print. Background:Pulsed field ablation (PFA) has emerged as an alternative to radiofrequency ablation. A contact force–sensing catheter was used to focally deliver PFA/radiofrequency at the pulmonary veins and other predefined sites in the atria.
In this large substudy of the AWARE Trial, a high-power short-duration (HPSD) radiofrequency ablation strategy was found to be similarly effective as a low-power long-duration strategy with no difference in time to first recurrence of any AF lasting ≥30 s. Methods Patients were grouped according to a HPSD (≥40 W) or LPLD (≤35 W) strategy.
a company primarily focused on leveraging its novel and proprietary CellFX Nanosecond Pulsed Field Ablation (nsPFA) technology for the treatment of atrial fibrillation, announced the completion of the first five procedures in its first-in-human feasibility study with its novel CellFX nsPFA cardiac catheter.
This study of 16 patients with persistent left superior vena cava (PLSVC) undergoing atrial fibrillation ablation shows a 66.7% identification rate of PLSVC-related triggers and an 85% success rate in acute isolation or targeted ablation. The recurrence rate of arrhythmia postablation was 46.7% However, a 46.7% years, 31.2%
Abstract Introduction During atrial fibrillation ablation (AFA), achievement of first pass isolation (FPI) reflects effective lesion formation and predicts long-term freedom from arrhythmia recurrence. We aim to determine the clinical and procedural predictors of pulmonary vein FPI.
Abstract Introduction Cryoballoon ablation (CBA) of the left atrial (LA) roof in addition to a pulmonary vein isolation has been expected to improve the clinical outcomes post-atrial fibrillation (AF) ablation. The 1-year Kaplan–Meier atrial arrhythmia free rate estimates were 80.6% C for Group A vs. −40.5 ± 7.5°C
We present the long-term outcome of catheter ablation (CA) and electrophysiological characteristics in HIV+ AF patients. During first procedure, all received isolation of pulmonary vein (PV) + posterior wall and superior vena cava. Among patients that underwent redo ablation non-PV triggers were higher in HIV group [93.5%
Pulmonary vein isolation (PVI) has been established as a cornerstone therapy for atrial fibrillation (AF). 1 Several studies have highlighted the significant role of non-pulmonary premature atrial complexes (non-PV PACs) in triggering AF/AT episodes.2,3
Abstract Introduction Despite advanced ablation strategies and major technological improvements, treatment of persistent atrial fibrillation (AF) remains challenging and the underlying pathophysiology is not fully understood. After a blanking period of 6 weeks, recurrence of any atrial arrhythmia was documented in 26 patients (52%).
Pulsed field ablation (PFA) is a novel modality shown to be safe and efficient.1 1 PFA is conventionally used for pulmonary vein isolation (PVI), but interest has arisen in delivering linear lesions to the posterior wall2 and mitral isthmus.3 3 The durability of these lesion sets has not been well evaluated.
David Newton , Clinical Cardiac Electrophysiologist at Memorial Health University Physicians Heart Care and Dr. Andrea Natale , Executive Medical Director at T exas Cardiac Arrhythmia Institute, St. David’s Medical Center. With this differentiated system, Biosense Webster is giving EPs the tools and information they need in real-time.
A 37-year-old woman with biventricular repair for pulmonary atresia and an intact ventricular septum was referred for an electrophysiological study in the context of recurrent atrial arrhythmias with multiple electrical cardioversions. Her clinical tachycardia was easily inducible and had a cycle length (TCL) of 340 ms.
The cyanosis in Ebstein’s anomaly, is usually not due to pulmonary hypertension, but because tricuspid regurgitation jet is directed across the atrial septal defect. This can be a source of cardiac arrhythmia as well. Electrophysiological study will show that, and this pathway can be ablated.
Crochetage sign on ECG in ASD ECG in ASD with severe pulmonary hypertension: Tall R’ in V1, ST depression in inferior leads and V2-V5, and T inversion in inferior leads and V1-V6 are seen. Fragmented QRS is a marker of myocardial scar and consequent arrhythmias in ischemic and nonischemic cardiomyopathy.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.









































Let's personalize your content