This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
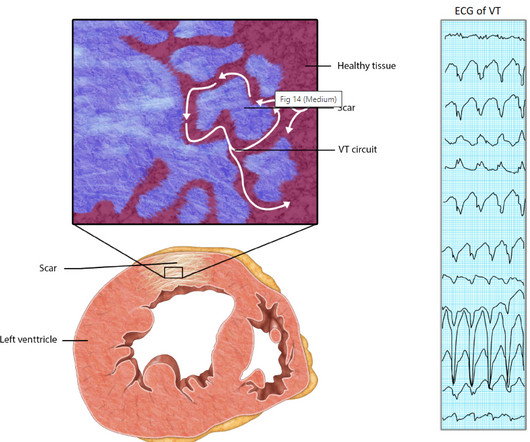
Ventricular tachycardia is a potentially life threatening cardiac arrhythmia. Monomorphic ventricular tachycardia in the setting of acute myocardial ischemia can also be treated by intravenous lignocaine bolus followed by infusion. If the rate is very fast, hemodynamic deterioration can occur rapidly.
Is there ischemia? Idioventricular rhythm is a common "reperfusion arrhythmia." ECG Diagnosis is either : 1) junctional rhythm with new LBBB, and possibly ischemia 2) accelerated idoventricular rhythm with possible ischemia, and possibly related to restoration of normal perfusion. But it is not conclusive.
Are you confident there is no ischemia? Primary VT , and the VT with tachycardia is causing ischemia with chest discomfort (supply-demand mismatch/type 2 MI)? Ischemia from ACS causing the chest discomfort, with VT another consequence (or coincidence)? Do you agree with this strategy? How can you better assess the ST segments?
While medical trial of an antiarrhythmic agent can at times be undertaken ( assuming the clinician remains at the bedside throughout the process ) — synchronized cardioversion is often favored for treatment of AFib with WPW, given the exceedingly rapid ventricular response with this arrhythmia. What do YOU see?
He got an MR, however that showed no scar or evidence of AVRD and he had a stress test with no evidence of inducible ischemia with almost 20 METs." It was ablated. == MY Comment , by K EN G RAUER, MD ( 6/28 /2023 ): == There is a tendency for clinicians to interpret cardiac arrhythmias in binary fashion.
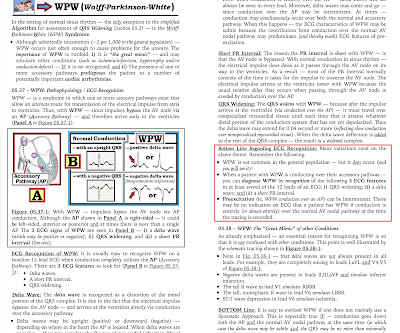
2] Conduction through the accessory pathway can be intermittent (with different degrees of pre-excitation), and affected by ischemia. 3] So a patient with WPW can have the pattern induced by ischemia, and there is also a report of a patient with pre-existing WPW which was “ablated” by myocardial infarction after an LAD occlusion.[4]
We see a regular tachycardia with a narrow QRS complex and no evidence of OMI or subendocardial ischemia. Even experienced providers make the mistake of using the term, “SVT” as a specific diagnosis — when in fact this generic term includes all arrhythmias in which the rate is “tachycardic” ( ie, ≥100 in an adult ).
The patient was found to have a "concealed" posteroseptal pathway (WPW without delta waves) confirmed to have SVT at EP study and was ablated. Here is the Electrophysilogist's note: "Only 1 pathway attachment could be ablated, the second one deep within the CS could not be ablated with high power.
Here is her post-cardioversion ECG: ECG#2 - Immediately post cardioversion: Appropriate ST depression maximal in V5-6 and lead II, secondary to subendocardial ischemia, likely residual from the preceding tachycardia. Radiofrequency ablation was performed for a right sided posteroseptal bypass tract. She was sedated and cardioverted.
However, he suddenly developed a series of malignant ventricular arrhythmias. Below are printouts of some of the arrhythmias recorded. There is no definite evidence of acute ischemia. (ie, This time, the arrhythmia did not spontaneously terminate — but rather degenerated to VFib, requiring defibrillation.
And superimposed subendocardial ischemia pattern, of course. Is this patient a candidate for cardioversion or ablation? ( If ablation is contemplated — definitive diagnosis will be made at EP study. ( While these do not alter emergency management of this patient's arrhythmia — They should be noted.
Relationship between Ischemia and arrhythmia While the relationship between Ischemia and VT is really complex, the term “Ischemic VT” itself adds more twists. Even here, it is the associated factors, like hypoxia or acidosis are the triggers which of course are resultant of Ischemia. Reference 1. 117.006120.
Can you ever think of ablating PVs in a patient with AF and COPD, where the right atrium is under stress and strain? Focus-less Atrial fibrillation Right from the days of James Mckenzie , when AF was refered to as delirium cordis or ataxia of pulse, AF was always considered as a chaotic, focus-less arrhythmia. Reference 1.
The possibility of an ischemic cause of the ventricular arrhythmia has to be considered! That said there were no clinical symptoms or ECG findings suggestive of ongoing ischemia. A workup was undertaken in search of a cause of the patient's ventricular arrhythmia. The patient has been scheduled for a PVC ablation procedure.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



















Let's personalize your content