This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Background Atrial arrhythmias (AA) and heart failure (HF) are major causes of hospitalisation in adult congenitalheartdisease (ACHD). Methods In this single-centre retrospective cohort study, data from 3995 patients with ACHD were analysed.
ABSTRACT Introduction Data regarding safety and long-term outcome of very high-power-short duration (vHPSD) ablation in adult congenitalheartdisease (ACHD) patients with paroxysmal or persistent atrial fibrillation (AF) are lacking. Regardless of CHD complexity, no vHPSD ablation modality related complications occurred.
Patients with adult congenitalheartdisease (ACHD) such as Tetralogy of Fallot (ToF) are at high risk for ventricular arrhythmias requiring ablation. Less common syndromes such as double outlet right ventricle (DORV) and Williams Syndrome provide additional complications.
All these features together in a cyanotic congenitalheartdisease is characteristic of tricuspid atresia. Fragmented QRS is a marker of myocardial scar and consequent arrhythmias in ischemic and nonischemic cardiomyopathy. Multiple accessory pathways can occur and radiofrequency catheter ablation is effective.
Patients with dextro-transposition of the great arteries (d-TGA) are at risk for recurrent atrial arrhythmias late after atrial switch operations. Advanced anatomic knowledge including prior surgical incisions are integral in planning the ablation procedure.
A 37-year-old woman with biventricular repair for pulmonary atresia and an intact ventricular septum was referred for an electrophysiological study in the context of recurrent atrial arrhythmias with multiple electrical cardioversions. Her clinical tachycardia was easily inducible and had a cycle length (TCL) of 340 ms.
Transcript of the video: Ebstein’s Anomaly is one of the cyanotic congenitalheartdisease in which survival to adult life is common. This can be a source of cardiac arrhythmia as well. Electrophysiological study will show that, and this pathway can be ablated.
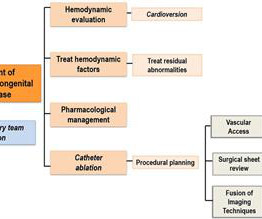
My understanding is that the decision was made for today's patient to be formally evaluated by EP cardiology with consideration given to ablation and/or insertion of an ICD ( I mplantable C ardioverter D efibrillator ). ECG Blog #422 and Blog #425 Cases with CongenitalHeartDisease in Adults.
The prevalence of congenitalheartdisease (CHD) in adult patients has risen with advances in diagnostic and surgical techniques. Patients with CHD commonly experience both supraventricular and ventricular arrhythmias, with each CHD type associated with different arrhythmia patterns.
Atrioventricular nodal reentrant tachycardia (AVNRT) is a common supraventricular tachycardia in children and congenitalheartdisease (CHD) patients. Nowadays, in large enough children, chronic treatment for symptomatic and recurrent AVNRT episodes relies on transcatheter ablation.
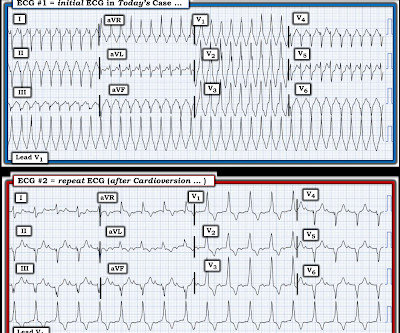
It would probably tell us whether the abnormal QRS morphology that we see in Figure-1 is the result of VT vs SVT ( ie, with the abnormal QRS morphology being the result of the patients underlying CongenitalHeartDisease ). ECG Blog #422 and Blog #425 — Cases with CongenitalHeartDisease in Adults.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

















Let's personalize your content