This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Ambulatory electrocardiography (ECG) monitoring revealed recurrent polymorphic ventricular tachycardia (PMVT). The patient presented with recurrent palpitations and pre-syncope, with no chest pain.
tim.hodson Mon, 03/31/2025 - 15:02 March 31, 2025 iRhythm Technologies, Inc. has announced results from two large real-world retrospective analyses presented at the American College of Cardiology (ACC) 2025 Scientific Sessions in Chicago. Long-term outcome of non-sustained ventricular tachycardia in structurally normal hearts.
Publication date: Available online 21 March 2025 Source: The American Journal of Cardiology Author(s): Wenchi Guan, Jun Liu, Yanbing Gu, Jianjun Li, Keping Chen, Yan Yao
Journal of the American Heart Association, Volume 14, Issue 4 , February 18, 2025. had ventricular tachycardia/ventricular fibrillation and 73.4% BackgroundInhospital cardiac arrest (IHCA) is associated with significant morbidity and mortality. Multivariable logistic regression analysis was used to adjust for potential confounders.
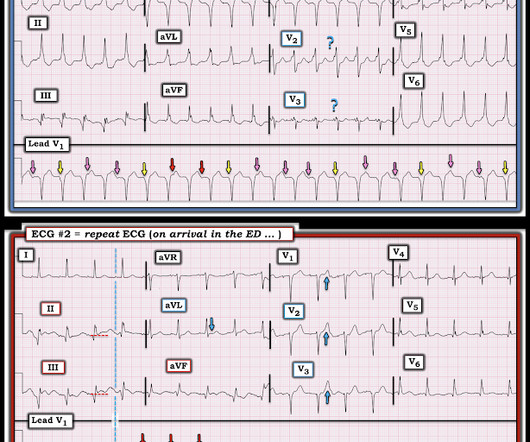
This proves AV dissociation, and by extension ventricular tachycardia. The note lists a diagnosis of "tachycardia," which is described as "narrow complex." (The Repeat ECG obtained in ER: Fortunately for the patient, his ventricular tachycardia spontaneously resolved. Documentation lists a diagnosis of "sinus tachycardia."
It is a wide complex regular tachycardia at a rate of 120. Is it ventricular tachycardia? I fear that many learners would also not easily recognize where the QRS actually ends, and I fear that some may think that this is ventricular tachycardia due to inability to distinguish QRS from ST segment. The ST Elevation is NOT typical.
The status of the patients chest pain at this time is unknown : EKG 1, 1300: There is sinus tachycardia and artifact of low and high frequency. However, there is also significant tachycardia , with heart rate of 116, and known hypoxia. She arrived to the ED with a nonrebreather mask. Her blood pressure on arrival was 153/69.
Landiolol Approval Date: November 22, 2024 Indication: Approved for the treatment of supraventricular tachycardia (SVT). Studies on Supraventricular Tachycardia : 5 studies , a total of 317 adults. Heart rate reduction within 10 minutes : Landiolol: 40%-90%.
TiCM is defined as the presence of a reversible form of LV dysfunction due solely to an increase in ventricular rate from any type of frequent or sustained tachycardia ( rapid AFib being the most common precipitating rhythm but TiCM has also been shown to arise from AFlutter, reentry SVT rhythms, ATach, frequent PVCs, episodes of VT ).
Smith comments : Wide complex tachycardia. The differential diagnosis of WCT is: 1) Sinus tachycardia with "aberrancy" (in this case RBBB and LAFB), but there are no P-waves and the QRS morphology is not typical of simple RBBB/LAFB. Also, if the rate is constant, not wavering up and down, it is highly unlikely to be sinus tachycardia.
QUESTION: This tracing was interpreted as sinus tachycardia with some kind of BBB ( B undle B ranch B lock ). ANSWER: There is no Bundle Branch Block because the rhythm is not sinus tachycardia. Thus, one might easily be fooled from Figure-1 into thinking that todays rhythm is sinus tachycardia. What kind of BBB is this?
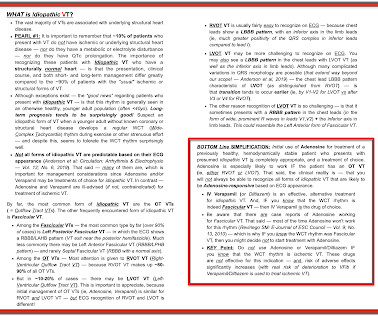
During observation in the ED the patient had multiple self-terminating runs of Non-Sustained monomorphic Ventricular Tachycardia (NSVT). This patient very likely has some form of idiopathic ventricular tachycardia. Of the ventricular outflow tract tachycardias (RVOT-VT) makes up 80-90%.
There was never ventricular fibrillation (VF) or ventricular tachycardia (VT), no shockable rhythm. Here is a similar case: Collapse, Ventricular Tachycardia, Cardioverted, Comatose on Arrival. Agitation, Confusion, and Unusual Wide Complex Tachycardia. There is sinus tachycardia at ~115/minute.
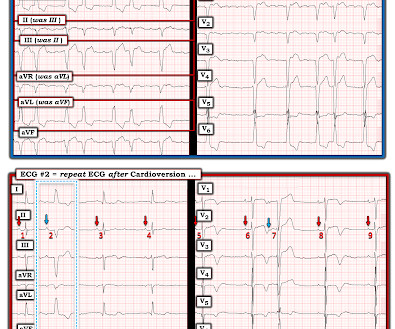
T wave inversion as seen in ECG #2 is not uncommon following a sustained tachyarrhythmia ( sometimes called a "Memory Effect" or "post-tachycardia" syndrome ). In most cases when not due to a new infarction this post-tachycardia T wave inversion resolves over the ensuing hours ( and almost alwlays within 1-2 days ).
Some OMI have zero ST elevation OMI can happen in young patients with no known medical history == MY Comment , by K EN G RAUER, MD ( 1/24 /2025 ): == There is a lot to be learned from today's post. In Figure-1 I facilitate comparison of the 3 ECGs in today's case by putting them together. This unfortunately is faulty reasoning.
In view of the clinical history ( ie, that this patient had a history of longstanding AFlutter but as far as we know, no chest pain ) this ST-T wave change most likely reflects a "memory" effect , in which there will often be ST-T wave abnormalities that persist for hours ( up to a few days ) following a long period of a sustained tachycardia.
Ventricular tachycardia?) This is why you should never wait for troponin to reperfuse when the ECG says "OMI [link] == MY Comment, by K EN G RAUER, MD ( 1/21/2025 ): == Todays case is frustrating because there is no way that 30 hours should have passed until cardiac cath was done. He said it felt like "someone ripped [his] heart out."
This ECG was recorded: It is difficult to appreciate P-waves, but I believe this is sinus tachycardia. In Figure-1 Ive labeled ECG #1 , which confirms Dr. Smiths suspicion of sinus tachycardia as the rhythm. BOTTOM Line: The rhythm in today's initial ECG is sinus tachycardia , with some variation in rate. He was put on BiPAP.
Awareness of our relative certainty about whether we are dealing with ischemic or idiopathic VT vs some form of SVT vs a WPW-related tachycardia can guide us for deciding when to try vagal maneuvers, electrical cardioversion, or some form of medical therapy ( ie, Adenosine, Amiodarone, Verapamil, -Blocker, or other ).
While its action improves AV conduction it may increase the sinus rate, producing a sinus tachycardia with adverse effect. A DDENDUM # 1 ( 3/8/2025 ) regarding the Term " O MI " The new terminology that I favor adds "OMI" ( = O cclusion-based M yocardial I nfarction ) to the classification of acute MI.
Drug toxicity , especially diphenhydramine , which has sodium channel blocking effects, and also anticholinergic effects which may result in sinus tachycardia, hyperthermia, delirium, and dry skin. If the QRS is prolonged, then the differential includes: 1. Hyperkalemia 2. Other drugs with sodium channel blockade: Tricyclic antidepressants.
2025.110515 [link] Abstract Objective: The administration of amiodarone or lidocaine is recommended during the resuscitation of out-of-hospital cardiac arrest (OHCA) patients presenting with defibrillation-refractory or recurrent ventricular fibrillation or ventricular tachycardia. DOI: 10.1016/j.resuscitation.2025.110515
link] == MY Comment , by K EN G RAUER, MD ( 1/20 /2025 ): == If you Google, Broken Heart Syndrome you will immediately see reference to many pages of Patient Education news briefs and informationals, in which the questions addressed are, Can You Really Die of a Broken Heart? & Dawson, D. Circulation , 145 (13), 10021019.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


























Let's personalize your content