This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
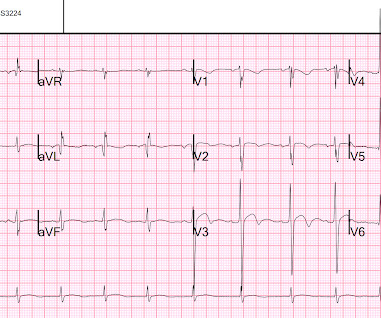
Theres ST elevation in V3-4 which meets STEMI criteria, which could be present in either early repolarization, pericarditis or injury. Lets see what happens in the current STEMI paradigm. Emergency physician: STEMI neg but with elevated troponin = Non-STEMI The first ECG was signed off. What do you think?
The emergency medicine physician documented, "His initial EKG is riddled with artifact and difficult to interpret but does not look like a STEMI." The ECG remains positive for STEMI by GE. The true AV groove LCx was "jailed" by the stent and appears occluded in the post PCI image. The emergency physician consulted cardiology.
Case submitted by Andrew Grimes, Advanced Care paramedic, with additions from Jesse McLaren and Smith An 84-year-old male with a notable cardiac history (CABG, multiple stents) woke at 0500hrs with pressure in his chest, diaphoresis, and light-headedness. STEMI criteria are only 43% sensitive for OMI.
He reports this was similar to how he felt when he had his heart attack 4 years prior, now s/p 4 stents. Note: the 2022 ACC Expert consensus Chest pain guidelines state that "posterior STEMI-Equivalent" is a sign of acute coronary occlusion. 2/3 of STEMI have a peak 4th generation troponin I greater than 10.0 NSTEMI-OMI").
He had undergone stenting of the LAD several weeks ago (unclear whether elective for stable symptoms, or in response to acute coronary syndrome). Acute chest pain, right bundle branch block, no STEMI criteria, and negative initial troponin. Written by Pendell Meyers An adult man presented with acute chest pain.
He has a history of coronary artery disease and a STEMI two years prior that was treated with primary PCI. At the time of this initial ED ECG, his symptoms were improving ECG #1 on admission to the ED The patient was not seen quickly in the ED as it was a busy shift and the ECG did not meet STEMI criteria. The below ECG was recorded.
This ECG pattern is my favorite example of how the STEMI criteria are fundamentally flawed. At cath there was a 100% proximal LAD occlusion, which was opened and stented. We have a series of 20 TIMI-0 LAD Occlusions that do meet STEMI criteria. There is a de Winter T- wave pattern also in lead I. Troponin T peaked at 9378 ng/L.
His first EKG is shown below, with a lead II rhythm strip: EKG 1, 1645 A provisder who is looking for STEMI would not see much in this EKG. It is possible that the T waves in this EKG are of an intermediate morphology between full-blown STEMI and inferior reperfusion. The thrombus was aspirated and the distal RCA was stented.
He has never been poisoned by the STEMI/NSTEMI paradigm because he has never been to medical school. The Queen of Hearts recognizes this as OMI ("STEMI/STEMI Equivalent"). It was treated with a drug eluting stent. He just graduated from college. He has no medical training, but he has read this blog for years. Lucky Hans.
Here is the prehospital ECG, recorded in the presence of pain: Hyperacute anterolateral STEMI The medics had activated the cath lab and the patient went for angiogram and had a 95% stenotic LAD with TIMI-3 flow. A stent was placed. Serial ECGs demonstrated dynamic changes diagnostic of ACS (transient STEMI) 4.
Written by Jesse McLaren An 80 year old with a history of CHF, ESRD on dialysis, and multiple prior cardiac stents presented to the emergency department with 3 days of intermittent chest pain and shortness of breath that resolved after nitro, which felt like prior episodes of angina. Discharge diagnosis was Non-STEMI.
Unfortunately, the ECG was interpreted as no significant change from prior , "no STEMI"!! Approximately 5 minutes after ROSC, this ECG was obtained (about 45 minutes after arrival): Obvious anterolateral OMI, and STEMI criteria positive for those who care or need it. He was sent back to the waiting room, where he suffered a VF arrest.
At 1210, the case was discussed with a cardiologist at a PCI capable facility, who accepted the patient for transfer, noting the ST depression in anterior leads as consistent with ischemia but not a STEMI. The proximal and mid LAD stenoses were stented and the OM 2 was left alone. 5 years later ( now in 2025 ) the problem remains.
After stent deployment, we often see improvement in the ST-T within seconds or minutes. Here is the final angiogram following placement of a stent in the ostial RCA. 2:04 PM, post stent deployment You can see that even after complete restoration of flow, the ECG still looks terrible, V most of all. & Dawson, D.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



















Let's personalize your content