This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
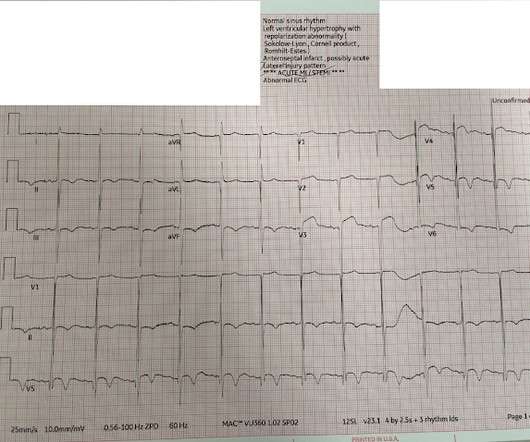
Even before we have clinical context, this ECG simply does not appear concerning for OMI, notwithstanding the machine's interpretation ** ** ACUTE MI / STEMI ** **. But in the world of STEMI, this is a challenging ECG to most. There were 80 positives by STEMI criteria, 88 by device algorithm, and 77 by AI software.
A 12-lead was recorded, showing "STEMI," but is unavailable. Moreover, if you know that catastrophic intracranial hemorrhage can result in an ECG that mimics STEMI, then you know that this patient probably has a severe intracranial hemorrhage. She was BVM ventilated and suctioned. Shortly thereafter, pulses were lost.
The lack of sufficient ST elevation to fulfill STEMI criteria may be the result of some pseudo-normalization following some spontaneous reperfusion of the "culprit" artery. F or M ore M aterial regarding ECG interpretation of OMIs ( that do not satisfy millimeter-based STEMI criteria ).
He has never been poisoned by the STEMI/NSTEMI paradigm because he has never been to medical school. His triage EKG is shown below: There is left bundle branch block, so the EKG must be evaluated for ischemia by Smith-modified Sgarbossa criteria. There is evidence of transmural ischemia of the posterior wall as well. Lucky Hans.
He has a history of coronary artery disease and a STEMI two years prior that was treated with primary PCI. At the time of this initial ED ECG, his symptoms were improving ECG #1 on admission to the ED The patient was not seen quickly in the ED as it was a busy shift and the ECG did not meet STEMI criteria. The below ECG was recorded.
It is not clear by her note what she meant by this (whether or not she recognized this EKG as diagnostic of transmural ischemia, and if so, of what territory) but emergent reperfusion therapy was not pursued. Subendocardial ischemia does not localize. At 1022, a troponin I (ref range <0.034 ng/mL) resulted at 4.437 ng/mL.
This ECG pattern is my favorite example of how the STEMI criteria are fundamentally flawed. We have a series of 20 TIMI-0 LAD Occlusions that do meet STEMI criteria. However, many patients with de Winter ECG pattern have TIMI 0 at angiography and the ECG pattern does not necessarily progress to STEMI. 17 have HATW. Under Review.
When interpreting ECGs such as the initial tracing in today's case We need to remember that we are not trying to "rule in" an acute STEMI. It is also the best way to miss a lot of acute OMIs in need of prompt cath with PCI ( ie, See recent publications by Ricci, Smith et al Ann Emerg Med, 2025 and McClaren, Smith et al JACC Adv.
STEMI criteria are only 43% sensitive for OMI. McLaren : The inferior T wave inversion suggests either reperfusion (if resolved symptoms) or subacute refractory ischemia and from the previous description of pain refractory to nitro it is likely the latter. Beware confusing the diagnosis of posterior STEMI by using posterior leads.
The ECG shows sinus tachycardia, RBBB+LAFB, and signs of anterolateral acute transmural ischemia (most likely due to acute coronary occlusion), with concordant STE in I and aVL, inappropriate STE in V4-6 (though limited a bit by motion, still definite). Near 100% mortality without rapid reperfusion."
PEARL # 3: Knowing there is an acute inferior STEMI I looked next to see if there is also acute posterior involvement ( which so often accompanies inferior MI ). But larger-than-expected Q waves in each of the inferior leads ( especially in lead III ) are probably the result of this patients ongoing acute inferior STEMI.
Supply-demand mismatch can cause ST Elevation (Type 2 STEMI). Also see these posts of Type II STEMI. An EKG from a year prior was available for comparison: The ED physician noted Initial EKG here read by the computer as a STEMI, however, there is a very poor baseline and a lot of artifact. See reference and discussion below.
Unfortunately, the ECG was interpreted as no significant change from prior , "no STEMI"!! Approximately 5 minutes after ROSC, this ECG was obtained (about 45 minutes after arrival): Obvious anterolateral OMI, and STEMI criteria positive for those who care or need it. He was sent back to the waiting room, where he suffered a VF arrest.
Severe ischemia can be present even when the chest pain is gone. Learning points: 40% of LAD OMI with TIMI-0 flow do NOT meet STEMI criteria (manuscript under consideration at Eur Ht. 20/53 did not meet STEMI criteria, but all showed OMI diagnosed by both Smith and the Queen of Hearts. The CLINICIAN is the historian.)
50% of LAD STEMI have Q-waves by one hour. Smith : In limb leads, the ST vector is towards lead II (STE lead II STE lead III, which is more likely with pericarditis than with STEMI). There were no other causes of dyspnea apparent and thus we can assume that myocardial ischemia started 6 days prior. See Raitt et al.:
Time 7 hours lead reversal There is limb lead reversal (QRS in I and aVL are now inverted), but nevertheless one can see that the ischemia appears to have resolved. Negative trops and negative angiogram does not rule out coronary ischemia or ACS. This is extremely elevated for a type 2 MI and totally consistent with STEMI.
How well does the computer interpretation perform? -- in this case, the computer diagnosed STEMI but the patient had Fever with Brugada -- A young F is hyperthermic, delirious, and dry: Fever-induced Brugada? Among potential conditions that may produce Brugada Phenocopy are infarction and ischemia. Ischemia or infarction.
It is possible there is microvascular dysfunction producing residual transmural ischemia. But this is most common when there is prolonged ischemia, and this patient had the fastest reperfusion imaginable! There was indication of parasympathetic overdrive ( the acute inferior STEMI with profound bradycardia and junctional escape ).
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
























Let's personalize your content