This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
If we took this as the gold standard, we would conclude that the computer interpretation was safe and accurate at least accurate enough to not miss STEMI, and that physicians should not be interrupted to interpret it, because there would be no change in patient management. The latest is Langlois-Carbonneau et al.
Stroke, Volume 56, Issue Suppl_1 , Page AWP317-AWP317, February 1, 2025. Introduction:Atrial fibrillation (AF), which can be easily identified through electrocardiogram (ECG), is a well-established predictor of ischemic stroke (IS) in comparison to other stroke subtypes. Analyses were conducted using R version 4.3.1.Results:In
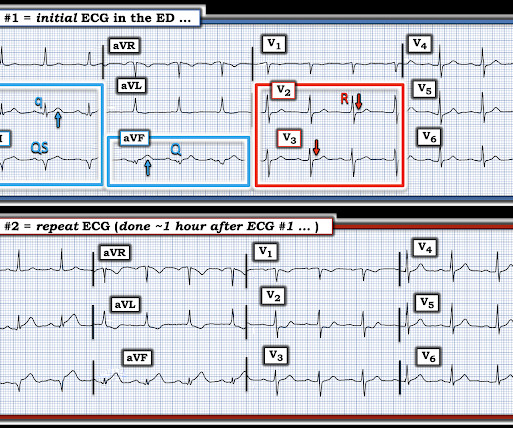
Here is the PMcardio Queen of Hearts interpretation of the ECG: STEMI equivalent detected. Inferior and posterior OMI without STEMI criteria. About an hour later another ECG was obtained: Barely meets STEMI criteria in inferior leads, but obvious inferior and posterior OMI. The cath lab was now activated for STEMI.
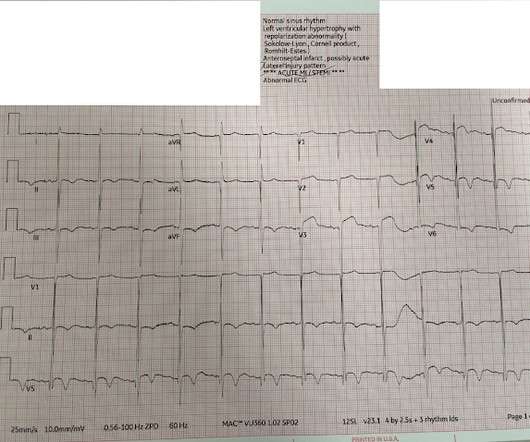
Even before we have clinical context, this ECG simply does not appear concerning for OMI, notwithstanding the machine's interpretation ** ** ACUTE MI / STEMI ** **. But in the world of STEMI, this is a challenging ECG to most. Artificial intelligence (AI) algorithms show promise to improve electrocardiogram (ECG) interpretation.
The de Winter electrocardiogram pattern is an infrequent presentation, reported to occur in 2% to 3.4% This ECG pattern is my favorite example of how the STEMI criteria are fundamentally flawed. We have a series of 20 TIMI-0 LAD Occlusions that do meet STEMI criteria. of patients with anterior myocardial infarction ( 1 ).
Peaked T waves: Hyperacute (STEMI) vs. Early Repolarizaton vs. Hyperkalemia Recognize subtle findings of hyperK and, if present, treat with Calcium immediately! Severe hyperkalemia: can the electrocardiogram risk stratify for short-term adverse events. HyperKalemia with Cardiac Arrest. References 1. Lindner et al. Durfey et al.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.











Let's personalize your content