This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
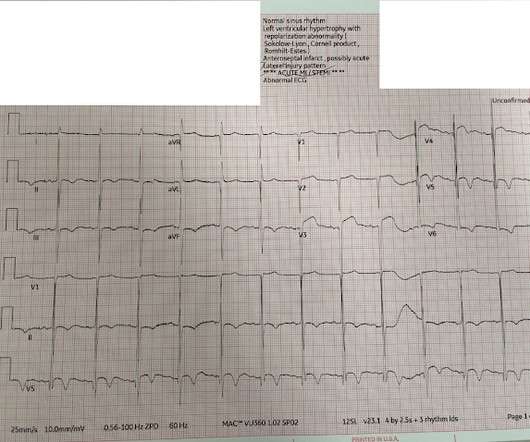
Written by Jesse McLaren A 50 year old presented to triage with one hour of chestpain, and the following ECG labeled normal by the computer (GE Marquette SL) algorithm. Smith comment: we showed that the first troponin, even in full-blown STEMI, is negative 25% of the time. What do you think?
Theres ST elevation in V3-4 which meets STEMI criteria, which could be present in either early repolarization, pericarditis or injury. Lets see what happens in the current STEMI paradigm. Emergency physician: STEMI neg but with elevated troponin = Non-STEMI The first ECG was signed off. Chestpain still persists.
He has a history of coronary artery disease and a STEMI two years prior that was treated with primary PCI. He contacted EMS due to acute onset chestpain and feeling unwell and fatigued. He subsequently developed worsening chestpain. Pain is improving and ischemic T-wave inversions are no longer present".
STEMI criteria are only 43% sensitive for OMI. He was given two separate sprays of nitroglycerin sublingually, neither of which improved his pain but did cause him to become briefly hypotensive ( 600 ng/L. The patient has acute persistent refrectory chestpain and elevated troponin. There is no need for another ECG.
Written by Hans Helseth A 34 year old man with no known medical history presented to the ED after an hour of chestpain. He described the pain as a mid sternal "burning sensation" and rated it 8.5 out of 10 at onset, but on presentation to the ED, reported that the pain had improved to 4.5. 10 chestpain.
Even before we have clinical context, this ECG simply does not appear concerning for OMI, notwithstanding the machine's interpretation ** ** ACUTE MI / STEMI ** **. But in the world of STEMI, this is a challenging ECG to most. There were 80 positives by STEMI criteria, 88 by device algorithm, and 77 by AI software.
He has never been poisoned by the STEMI/NSTEMI paradigm because he has never been to medical school. Case A 76 year old man with chronic hypertension but no history of coronary disease or myocardial infarction presented to the ED with chestpain at 2343. The Queen of Hearts recognizes this as OMI ("STEMI/STEMI Equivalent").
Written by Pendell Meyers, sent by anonymous, with additions by Smith A man in his 40s had acute chestpain and called EMS. Here is the PMcardio Queen of Hearts interpretation of the ECG: STEMI equivalent detected. Inferior and posterior OMI without STEMI criteria. The cath lab was now activated for STEMI.
Scenario 1 : The patient presents with 24 hours of substernal chestpain. 50% of LAD STEMI have Q-waves by one hour. Smith : In limb leads, the ST vector is towards lead II (STE lead II STE lead III, which is more likely with pericarditis than with STEMI). He presented to the emergency department for evaluation.
A 50-something male presented to triage with chestpain for one day. A Chest X-ray showed infiltrates. Thus, another etiology of chestpain is found, and the fever suggests "fever-induced Brugada." The presenting complaint noted at Triage was, "a 50yo man with chestpain!" The temperature was 39.5
The patient received three nitroglycerin tablets with significant "improvement" in his chestpain. Improved chestpain is unresolved chestpain. I am commonly told, and I commonly read in the chart that chestpain is resolved. It is not enough for the chestpain to be "much better."
Written by Pendell Meyers An adult man presented with acute chestpain. Acute chestpain, right bundle branch block, no STEMI criteria, and negative initial troponin. What is the Diagnosis in this 70-something with ChestPain? 68 minutes with chest compressions, full recovery.
A 50 something male presented in the evening to ED for evaluation of chestpain that started at 1600. Note: the 2022 ACC Expert consensus Chestpain guidelines state that "posterior STEMI-Equivalent" is a sign of acute coronary occlusion. The chestpain continued for hours. NSTEMI-OMI").
The emergency medicine physician documented, "His initial EKG is riddled with artifact and difficult to interpret but does not look like a STEMI." This is a very bold statement in a type 1 diabetic with very concerning sounding chestpain. The patient was treated with aspirin and a GI cocktail, which did not help the pain.
Written by Willy Frick A man in his 60s with a history of hypertension and 40 pack-year history presented to the ER with 1 day of intermittent, burning substernal chestpain radiating into both arms as well as his back and jaw. In the world of STEMI, we are incapable of recognizing the first ECG as a false negative.
A 30 year old African American Male presented to the ED with chestpain that occurred the day before. There was no pain on the day of presentation. 2019.06.007) (Full text here: [link] ) The ECG above is diagnostic of Wellens' syndrome (full reference below): 1) Episode of anginal chestpain that is resolved (GONE!)
The patient contacted the ambulance service after he experienced sudden onset chestpain and diaphoresis that had started 20 minutes prior. This ECG pattern is my favorite example of how the STEMI criteria are fundamentally flawed. We have a series of 20 TIMI-0 LAD Occlusions that do meet STEMI criteria. 17 have HATW.
No chestpain. Im changed. == MY Comment , by K EN G RAUER, MD ( 1/16 /2025 ): == It's not often that we see a clinical entity for which it seems that the patient "read the textbook" before the ECG was recorded. hs Trop I is 15,000. I think it is OMI. Taking her to the cath lab. He wrote: OMI it was. Large diagonal. Now opened.
The ECG in Figure-1 was obtained from a middle-aged man who presents to the ED ( E mergency D epartment ) with 6 hours of chestpain. Figure-1: The initial ECG in today's case obtained from a middle-aged man with 6 hours of chestpain. ( He is hemodynamically stable.
A 69 year old woman with a history of hypertension presented to the emergency department by EMS for evaluation of chestpain and shortness of breath. She awoke in the morning with sharp chestpain which worsened throughout the morning. As her pain worsened, so did her dyspnea. Also see these posts of Type II STEMI.
Written by Jesse McLaren An 80 year old with a history of CHF, ESRD on dialysis, and multiple prior cardiac stents presented to the emergency department with 3 days of intermittent chestpain and shortness of breath that resolved after nitro, which felt like prior episodes of angina. The patient had no further episodes of chestpain.
He denied chestpain. It is correct that he did not have chestpain, but we must remember that fully 1/3 of full blown STEMI do not present with chestpain. This is extremely elevated for a type 2 MI and totally consistent with STEMI. He had acute onset of shortness of breath.
A 62 year old man with hyperlipidemia presented to a rural emergency department with 7 hours of 3/10 chestpain. At 1210, the case was discussed with a cardiologist at a PCI capable facility, who accepted the patient for transfer, noting the ST depression in anterior leads as consistent with ischemia but not a STEMI.
Written by Pendell Meyers A man in his 60s presented with acute chestpain. Unfortunately, the ECG was interpreted as no significant change from prior , "no STEMI"!! Long term outcome is not available. == MY Comment, by K EN G RAUER, MD ( 2/1/2025 ): == We need to learn from cases like today's.
He had no chestpain, dyspnea, or any other anginal equivalent, and his vital signs were normal. There was indication of parasympathetic overdrive ( the acute inferior STEMI with profound bradycardia and junctional escape ). & Dawson, D. Takotsubo syndrome: Pathophysiology, emerging concepts, and clinical implications.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



























Let's personalize your content