This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Dr. Yang is also winner of the SCCT Best Abstract Award for his submission, “Coronary CT Angiography-derived Precursors Of Acute Coronary Syndrome In Ischemia-causing Lesions.” The SCCT Best Abstract Award is supported by the Cardiovascular Research Foundation of Southern California (CVRF of So.
He contacted EMS due to acute onset chestpain and feeling unwell and fatigued. He subsequently developed worsening chestpain. This, in the context of worsening chestpain , is evidence of reocclusion of the infarct-related artery and active OMI in development. The below ECG was recorded. What do you think?
He was given two separate sprays of nitroglycerin sublingually, neither of which improved his pain but did cause him to become briefly hypotensive ( 600 ng/L. The patient has acute persistent refrectory chestpain and elevated troponin. There is no need for another ECG. Just go to the cath lab!
Case A 76 year old man with chronic hypertension but no history of coronary disease or myocardial infarction presented to the ED with chestpain at 2343. His triage EKG is shown below: There is left bundle branch block, so the EKG must be evaluated for ischemia by Smith-modified Sgarbossa criteria.
Scenario 1 : The patient presents with 24 hours of substernal chestpain. Denying patients the potential benefit of revascularization just because their symptoms have lasted a certain amount of time shows poor understanding of the pathophysiology of myocardial ischemia. He presented to the emergency department for evaluation.
A 50-something male presented to triage with chestpain for one day. A Chest X-ray showed infiltrates. Thus, another etiology of chestpain is found, and the fever suggests "fever-induced Brugada." The presenting complaint noted at Triage was, "a 50yo man with chestpain!" Ischemia or infarction.
She did not even need to ask in this case, because even if the patient presented with chestpain, she would call it NEGATIVE. This ST-T wave pattern in lead V5 is not seen in other leads, as would be expected if this was truly a change of acute ischemia. What about the R = S Phenomenon in the Inferior Leads?
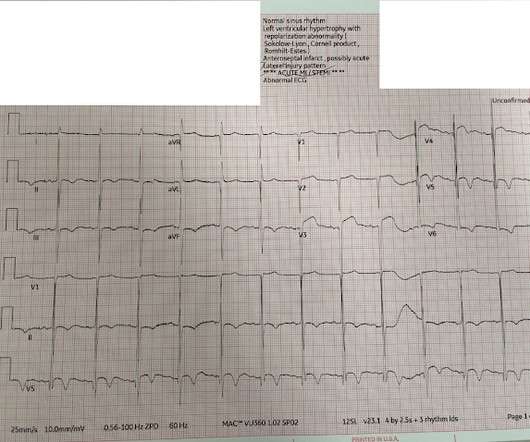
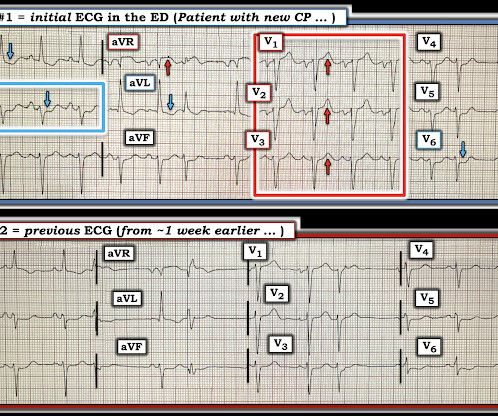
"Hi Steve wonder what you think of this ecg in a 60 yo woman w cp, known CAD" Presentation ECG (ECG 1): Here is her previous from one week prior when she presented with heart failure and trops were "negative" (ECG 2): My response: "They both look like active ischemia. The previous ECG also shows active ischemia."
The patient received three nitroglycerin tablets with significant "improvement" in his chestpain. Improved chestpain is unresolved chestpain. I am commonly told, and I commonly read in the chart that chestpain is resolved. It is not enough for the chestpain to be "much better."
Written by Pendell Meyers An adult man presented with acute chestpain. The ECG shows sinus tachycardia, RBBB+LAFB, and signs of anterolateral acute transmural ischemia (most likely due to acute coronary occlusion), with concordant STE in I and aVL, inappropriate STE in V4-6 (though limited a bit by motion, still definite).
A 69 year old woman with a history of hypertension presented to the emergency department by EMS for evaluation of chestpain and shortness of breath. She awoke in the morning with sharp chestpain which worsened throughout the morning. As her pain worsened, so did her dyspnea. This was written by Hans Helseth.
A 62 year old man with hyperlipidemia presented to a rural emergency department with 7 hours of 3/10 chestpain. It is not clear by her note what she meant by this (whether or not she recognized this EKG as diagnostic of transmural ischemia, and if so, of what territory) but emergent reperfusion therapy was not pursued.
The patient contacted the ambulance service after he experienced sudden onset chestpain and diaphoresis that had started 20 minutes prior. The above ECG is from man in his 80s with crushing chestpain. Transient ischemia may lead to "stunning". The ECG below ECG was recorded on the scene. References: Kloner, R.
Written by Willy Frick A woman in her 60s with very severe hyperlipidemia (LDL >200 mg/dL) presented with acute onset chestpain. She described the pain as moderate in severity, and said it had come and gone several times over the next few hours before ultimately resolving. Her symptoms began while getting off the bus.
The ECG in Figure-1 was obtained from a middle-aged man who presents to the ED ( E mergency D epartment ) with 6 hours of chestpain. Figure-1: The initial ECG in today's case obtained from a middle-aged man with 6 hours of chestpain. ( He is hemodynamically stable. They lead you to numerous posts with more on OMIs.
He denied chestpain. Time 7 hours lead reversal There is limb lead reversal (QRS in I and aVL are now inverted), but nevertheless one can see that the ischemia appears to have resolved. Negative trops and negative angiogram does not rule out coronary ischemia or ACS. Next day, with K = 4.6 The evidence of OMI is gone.
Written by Pendell Meyers A man in his 60s presented with acute chestpain. Long term outcome is not available. == MY Comment, by K EN G RAUER, MD ( 2/1/2025 ): == We need to learn from cases like today's. This distinction is further complicated because marked LVH may at times mask the ST-T wave changes of acute ischemia.
It is possible there is microvascular dysfunction producing residual transmural ischemia. But this is most common when there is prolonged ischemia, and this patient had the fastest reperfusion imaginable! He had no chestpain, dyspnea, or any other anginal equivalent, and his vital signs were normal. & Dawson, D.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






















Let's personalize your content