This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
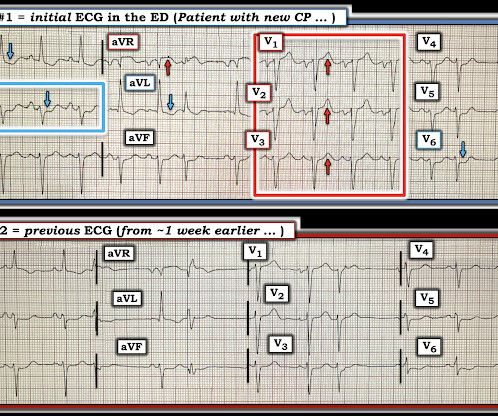
"Hi Steve wonder what you think of this ecg in a 60 yo woman w cp, known CAD" Presentation ECG (ECG 1): Here is her previous from one week prior when she presented with heart failure and trops were "negative" (ECG 2): My response: "They both look like active ischemia. The previous ECG also shows active ischemia." Just awful all around.
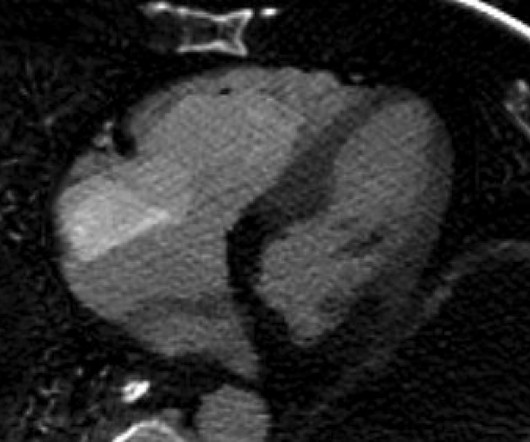
There is Transmural ischemia of Occlusion MI. Spectral CT This spectral CT image really highlights the dense transmural ischemia of the posterior wall. Here you can also see that there is dense ischemia of the RV. Assessment : Cardiology thought this was cardiogenicshock from RV dysfunction.
There is low voltage in the precordium which always makes reading ischemia harder. In ACS, chest pain is the warning sign of ongoing ischemia. Smith : As Willy says, and as we've said many times before, morphine will resolve pain without resolving ischemia. ECG 1 What do you think? To me, this ECG is not diagnostic.
Whenever there is tachycardia, I am skeptical of OMI unless it has led to severely compromised ejection fracction with cardiogenicshock. The patient was started on heparin for possible NSTEMI vs demand ischemia. increasing stenosis, ischemia, volume changes, increased blood pressure, atrial fibrillation, etc.)
The ECG shows sinus tachycardia, RBBB+LAFB, and signs of anterolateral acute transmural ischemia (most likely due to acute coronary occlusion), with concordant STE in I and aVL, inappropriate STE in V4-6 (though limited a bit by motion, still definite). Near 100% mortality without rapid reperfusion." The ST Elevation is NOT typical.
Anyone who has seen and studied OMI patients knows that this patient with proximal LAD pattern, with super high risk ischemic RBBB, and tachycardia, is in cardiogenicshock until proven otherwise. This pattern has very high mortality. The Emergency Physician contacted the Cardiologist immediately asking for cath lab activation.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.











Let's personalize your content