This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
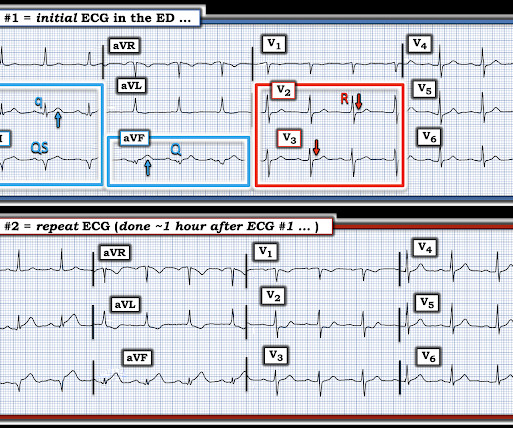
Unfortunately, the ECG was interpreted as no significant change from prior , "no STEMI"!! He was sent back to the waiting room, where he suffered a VF arrest. Approximately 5 minutes after ROSC, this ECG was obtained (about 45 minutes after arrival): Obvious anterolateral OMI, and STEMI criteria positive for those who care or need it.
Here is the PMcardio Queen of Hearts interpretation of the ECG: STEMI equivalent detected. Inferior and posterior OMI without STEMI criteria. About an hour later another ECG was obtained: Barely meets STEMI criteria in inferior leads, but obvious inferior and posterior OMI. The cath lab was now activated for STEMI.
A 12-lead was recorded, showing "STEMI," but is unavailable. The patient was unconscious BEFORE the cardiacarrest, at the same time that she had strong pulses. Therefore, cardiacarrest is NOT the etiology of the coma. She was BVM ventilated and suctioned. Shortly thereafter, pulses were lost.
Acute chest pain, right bundle branch block, no STEMI criteria, and negative initial troponin. Plus recommendations from a 5-member panel on cardiacarrest. Plus recommendations from a 5-member panel on cardiacarrest. These are often VERY difficult to recognized. Protocols can be overridden by Physician Judgment.
2] Curiously, ACLS does not include consideration of calcium in its bradycardia algorithm, which could have prevented the arrest and which along with the epi produced ROSC. HyperKalemia with CardiacArrest. regardless of the ECG (when the repeat level came back).[1] References 1. Lindner et al. West J Emerg Med 2017.
Unexplained cardiacarrest or documented VF/polymorphic VT: +3 3. Unexplained sudden cardiac death (3 categories) (+0.5 - +2) 4. Cardiacarrest. Clinical History 2.a. of atrial fib/flutter at age less than 30: +0.5 syncope of unclear etiology: +1 2.c. Suspected arrhythmic syncope: +2 2.d. Family History 3.a.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.












Let's personalize your content