This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
The 2025 AHA Statistical Update is the product of a full years worth of effort in 2024 by dedicated volunteer clinicians and scientists, committed government professionals, and AHA staff members.
The buzz around artificial intelligences impact on cardiology keeps growing louder, and thats proving to be particularly true in the AI-ECG segment, with 2025 already off to a strong start from ECG startups and researchers alike. The post AI-ECGs 2025 Kickoff appeared first on Cardiac Wire.
Stroke, Volume 56, Issue Suppl_1 , Page ATMP108-ATMP108, February 1, 2025. Introduction:Brain injury is the main cause of death and disability post-cardiacarrest, and hypoxic-ischemic brain injury (HIBI) severity is associated with poor outcomes. Patients with MRI in the first 7 days after cardiacarrest were included.
Publication date: Available online 9 March 2025 Source: The American Journal of Cardiology Author(s): Abdullah Naveed Muhammad, Sivaram Neppala, Himaja Dutt Chigurupati, Ahila Ali, Muhammad Omer Rehan, Sowjanya Kapaganti, Rabia Iqbal, Mushood Ahmed, Yasar Sattar, Jamal S. Rana, Gregg C. Fonarow, Sourbha Dani
Circulation: Cardiovascular Interventions, Volume 18, Issue 1 , Page e014499, January 1, 2025. The primary outcome was a composite of 30-day mortality, resuscitated cardiacarrest, hemodynamic instability, and 90-day readmission. Patients were divided into early (<12 hours) and delayed CBT (12 hours) groups.
Stroke, Volume 56, Issue Suppl_1 , Page A62-A62, February 1, 2025. Eligible patients were adults (>=18) admitted with ischemic stroke, intracerebral hemorrhage, or coma after cardiacarrest as the primary reason for hospitalization and who met at least one severity criteria (e.g. NIHSS 10 on day 2).
Stroke, Volume 56, Issue Suppl_1 , Page ATP261-ATP261, February 1, 2025. Introduction:Pediatric heart transplant (PHT) recipient survival has improved. Yet, neurologic morbidity related to heart failure and its treatment persist. Additionally, 38(45%) were ischemic and 34(40%) were hemorrhagic strokes.Of
Chugh, the Pauline and Harold Price Chair in Cardiac Electrophysiology Research at Cedars-Sinai, investigates the causes of and potential treatments for abnormal heart rhythms, including sudden cardiacarrest. 24 that will bring together participants in the 2025 Clinical Trials Research (CTR) program. 24: Christine M.
Stroke, Volume 56, Issue Suppl_1 , Page AWP373-AWP373, February 1, 2025. Cardiacarrest (CA) often leads to severe memory impairment, largely due to extensive neuronal loss in brain areas critical for cognitive function, including the hippocampus and amygdala.
Journal of the American Heart Association, Volume 14, Issue 4 , February 18, 2025. BackgroundInhospital cardiacarrest (IHCA) is associated with significant morbidity and mortality.
Stroke, Volume 56, Issue Suppl_1 , Page ADP59-ADP59, February 1, 2025. Intro:Mild hypothermia has proved clinically effective at improving outcomes in cardiacarrest patients for decades. Similarly, mild hypothermia has been shown to be neuroprotective in experimental stroke models. shiver response).
Smith comment: The patient was lucky to have a cardiacarrest. By undergoing an arrest, providers became aware of his OMI which had not been noticed on his diagnostic ECG, and he thus has a chance at some myocardial salvage. Had he not had one, he would have sat in the waiting room until his entire myocardium at risk infarcted.
Plus recommendations from a 5-member panel on cardiacarrest. Chest Pain and Right Bundle Branch Block == MY Comment , by K EN G RAUER, MD ( 1/9 /2025 ): == As per Dr. Meyers Today's initial ECG represents a "Must Recognize!" Acute chest pain, right bundle branch block, no STEMI criteria, and negative initial troponin.
The patient was unconscious BEFORE the cardiacarrest, at the same time that she had strong pulses. Therefore, cardiacarrest is NOT the etiology of the coma. More cases here to highlight: [link] Middle Aged Woman with Asystolic CardiacArrest, Resuscitated: Cath Lab?
2] Curiously, ACLS does not include consideration of calcium in its bradycardia algorithm, which could have prevented the arrest and which along with the epi produced ROSC. HyperKalemia with CardiacArrest. regardless of the ECG (when the repeat level came back).[1] References 1. West J Emerg Med 2017. Farkas et al.
This may be a sign of cardiac "stunning" following an MI or cardiacarrest ( See ECG Blog #272 for more on Causes of Low Voltage ). A series of 3 challenging tracings with QRS widening ( See My Comment at the bottom of the page in the March 6, 2025 post on Dr. Smith's ECG Blog ).
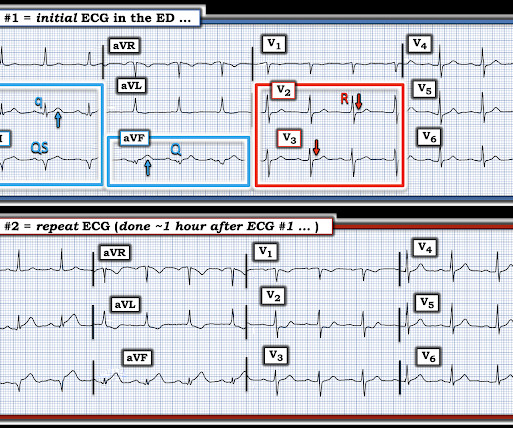
We are lucky this patient did not have a cardiacarrest while in the Waiting Room. Why this Patient should NOT be sent to the Waiting Room: After hearing the history and seeing the initial ECG in Figure-1 todays patient was sent to the Waiting Room. Instead ( as per Dr. Meyers ) worrisome ECG findings were evident on the initial ECG.
A retrospective 'target trial emulation' comparing amiodarone and lidocaine for adult out-of-hospital cardiacarrest resuscitation. Add to this the sobering clinical reality of how difficult it is to get objective, controlled, prospective data in the emergency situation of cardiacarrest and life-threatening arrhythmias.
In just 90 minutes from presentation, the patient progressed from that very subtle ECG to cardiacarrest. Discussion: This is a case of an initial ECG showing very subtle signs of hyperkalemia. Dr. McLaren recently wrote an excellent blog post on a similar case. Physician also reads it as normal) This is on a previous visit with K = 6.6:
They felt that the asystolic arrest suggested a different etiology of cardiacarrest. With the severe acidosis and absence of ST elevation, they felt there was more likely to be a non-cardiac etiology of his presentation.
Unexplained cardiacarrest or documented VF/polymorphic VT: +3 3. Unexplained sudden cardiac death (3 categories) (+0.5 - +2) 4. Cardiacarrest. Clinical History 2.a. of atrial fib/flutter at age less than 30: +0.5 syncope of unclear etiology: +1 2.c. Suspected arrhythmic syncope: +2 2.d. Family History 3.a.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



























Let's personalize your content