This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
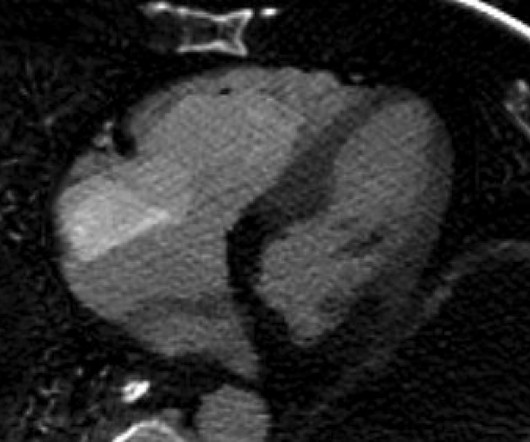
His rhythm on telemetry seemed to be sinus bradycardia vs junctional rhythm. There is Transmural ischemia of Occlusion MI. Spectral CT This spectral CT image really highlights the dense transmural ischemia of the posterior wall. Here you can also see that there is dense ischemia of the RV. What do you think?
Despite the baseline artifact theres sinus bradycardia, convex ST elevation in III, reciprocal ST depression in aVL and possible anterior ST depression indicating inferoposterior OMI. Still, an ECG was obtained at 0649hrs: (Digitized by PM Cardio) McLaren: The patient has a high pretest probability based on age, risk factors and symptoms.
Two more Cases of Takotsubo Stress Cardiomyopathy == MY Comment , by K EN G RAUER, MD ( 2/20 /2025 ): == Today's case provides an insightful example of how the History even more than the ECG made the diagnosis. Agitation, Confusion, and Unusual Wide Complex Tachycardia. What is it, why did it occur, and how to treat?
That said there were no clinical symptoms or ECG findings suggestive of ongoing ischemia. Below in Figure-5 is a 10-minute continuous lead II recording on oral Flecainide, now showing sinus bradycardia without a single PVC! You have given IV MgSO4 a fast acting -blocker and IV amiodarone bolus and infusion. No PVCs are seen.
Within ten minutes, she developed bradycardia, hypotension, and ST changes on monitor. Bradycardia and heart block are very common in RCA OMI. It is possible there is microvascular dysfunction producing residual transmural ischemia. He told the patient this horrible news. The other point in favor of RCA is junctional rhythm.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.











Let's personalize your content