This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
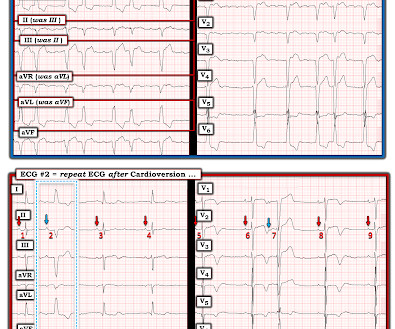
Despite the baseline artifact theres sinus bradycardia, convex ST elevation in III, reciprocal ST depression in aVL and possible anterior ST depression indicating inferoposterior OMI. He was given two separate sprays of nitroglycerin sublingually, neither of which improved his pain but did cause him to become briefly hypotensive ( 600 ng/L.
A man in his early 30s was walking when he developed central chestpain which was non-radiating, then had a syncopal event with bowel incontinence, and when he woke up he had ongoing chestpain. Notes never having symptoms like this before, pain is so severe its causing SOB. He called 911. As I wrote in that Nov.
He then provided some history: " Classic story for angina, few hours of crushing chestpain." For an example of how it can happen that potential false negative cardiac caths occur Check out the March 17, 2025 post. The rhythm is sinus bradycardia at ~55-60/minute. They do not recognize these patterns.
PEARL # 2: Did you notice in the post-conversion tracing that there is ST segment coving with fairly deep T wave inversion in the chest leads? Clinical correlation, and possibly Troponin levels are needed to determine whether this deep T wave inversion needs additional evaluation ).
Within ten minutes, she developed bradycardia, hypotension, and ST changes on monitor. Bradycardia and heart block are very common in RCA OMI. He had no chestpain, dyspnea, or any other anginal equivalent, and his vital signs were normal. He told the patient this horrible news. & Dawson, D.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.











Let's personalize your content