This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Cardiac arrest #3: ST depression, Is it STEMI? or is he an ACCESS Trial Candidate? == MY Comment , by K EN G RAUER, MD ( 7/5 /2024 ): == Clinical ECG interpretation is a 2-Step process. Description of today's ECG findings ( Sinus tachycardia with diffuse ST depression and ST elevation in aVR ) — is diagnostic of DSI.
== MY Comment , by K EN G RAUER, MD ( 8/30 /2024 ): == I was sent the ECG shown in Figure-1 — knowing only that the patient was being seen in the ED ( E mergency D epartment ). when the usual negative P wave deflection of sinus tachycardia is nowhere to be found in lead V1 )? This essentially rules in sinus tachycardia. (
My New E CG P odcasts ( 5/28/2024 ): These podcasts are part of the Mayo Clinic Cardiovascular CME Podcasts Series ( "Making Waves" ) — hosted by Dr. Anthony Kashou. 25:00 — The advantage of getting a 12-lead in an unknown tachycardia = “12 Leads are Better than One” ( = You have 12 leads to tell if the QRS is wide or narrow! ).
The conventional machine algorithm interpreted this ECG as STEMI. It shows sinus tachycardia with right bundle branch block. Taking a step back , remember that sinus tachycardia is less commonly seen in OMI (except in cases of impending cardiogenic shock). When EMS found her, she was dyspneic and diaphoretic. Both were wrong.
Prompt cath is therefore advised if the post-ROSC shows an acute STEMI. The rhythm is regular — at a rate just over 100/minute = sinus tachycardia ( ie, the R-R interval is just under 3 large boxes in duration ). Continuing with assessment of ECG #1 in Figure-2: The rhythm is sinus tachycardia at ~110/minute.
This certainly looks like an anterior STEMI (proximal LAD occlusion), with STE and hyperacute T-waves (HATW) in V2-V6 and I and aVL. How do you explain the anterior STEMI(+)OMI immediately after ROSC evolving into posterior OMI 30 minutes later? This caused a type 2 anterior STEMI. This prompted cath lab activation.
So this NSTEMI was likely a STEMI(-)OMI with delayed reperfusion. The patient was admitted as ‘NSTEMI’ which is supposed to represent a non-occlusive MI, but the underlying pathophysiology is analogous to a transient STEMI. West J Emerg Med 2024). Fortunately the patient did not reocclude while awaiting the angiogram.
Sinus tachycardia has many potential causes. This is especially true for the elderly patient with sinus tachycardia. What is the cause of the sudden tachycardia? It has been estimated that in the aggregate, they occur at a rate of about 3 per 1000 patients with acute MI, and most of these events occur in patients with STEMI.
The prehospital and ED computer interpretation was inferior STEMI: There’s normal sinus rhythm, first degree AV block and RBBB, normal axis and normal voltages. The paramedic notes called STEMI into question: “EMS disagree with monitor for STEMI callout. Vitals were normal except for oxygen saturation of 94%. Vitals were normal.
A prehospital “STEMI” activation was called on a 75 year old male ( Patient 1 ) with a history of hyperlipidemia and LAD and Cx OMI with stent placement. The two cases were considered: Patient 1 was recognized by the ED provider and the cardiologist as having resolved “STEMI”. He wrote most of it and I (Smith) edited. It was stented.
for those of you who do not do Emergency Medicine, ECGs are handed to us without any clinical context) The ECG was read simply as "No STEMI." Accessed May 28, 2024. and tachycardia, 1.8. Finally , they found that S1Q3T3, precordial T-wave inversions V1-V4, and tachycardia were independent predictors of PE.
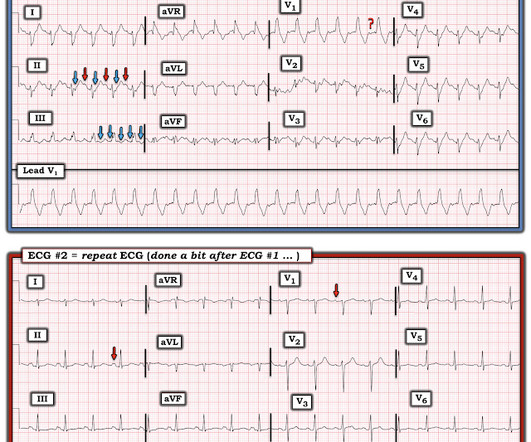
The ECG shows obvious STEMI(+) OMI due to probable proximal LAD occlusion. This progressed to electrical storm , with incessant PolyMorphic Ventricular Tachycardia ( PMVT ) and recurrent episodes of Ventricular Fibrillation ( VFib ). The below ECG was recorded. He required multiple defibrillations within a period of a few hours.
Automatic activity refers to enhanced pacemaking function (typically from a non sinus node source), for example atrial tachycardia. The receiving emergency physician consulted with interventional cardiology who stated there was no STEMI. Is there STEMI? The patient continued having chest pain. What is the rhythm? Moffat, M.
It definitely does not fulfill STEMI criteria, and I would argue that it would not lead to cath lab activation in most centers. NOTE #1: Sinus tachycardia is not usually seen in an uncomplicated acute MI. . == Below is the ECG of Patient #2 — as interpreted by the QOH. The ECG is diagnostic of occlusion myocardial infarction (OMI).
At 2111, the troponin I peaked at 12.252 ng/mL (this is in the range of STEMI patients, quite high). The conventional computer algorithm called “ sinus tachycardia, otherwise normal EKG ”. The patient received a diagnosis of “NSTEMI” and angiography was scheduled for the next day.
Easy LINK — [link] — My New E CG P odcasts ( 5/28/2024 ): These podcasts are part of the Mayo Clinic Cardiovascular CME Podcasts Series ( "Making Waves" ) — hosted by Dr. Anthony Kashou. 22:25 — What if you have a regular SVT ( = narrow-complex tachycardia ) without obvious P waves? ( speed should be optimal for you! ). 2:00 — Dr.
But for those wanting a "simpler" approach" — Consider the following ( which I review below in my ADDENDUM ): This patient is in a wide, "ugly-looking" and seemingly regular tachycardia without P waves. BOTTOM Line: The ECG in Figure-4 shows an extensive infero-postero-lateral STEMI.
It was read by the treating physician and the overreading cardiologist as "Paced, no STEMI." As the troponin T was 1521 ng/L (peak troponin T over 1000 ng/L is typical of STEMI) and still rising, no further troponins were measured. Did YOU Notice that the underlying rhythm in Figure-1 appears to be atrial tachycardia?
Final Diagnosis: "STEMI" (of course, as you can see in the ECGs above, this is not true, by definition this was NSTEMI. But the "final diagnosis" commonly just reflects whether the patient was given emergent therapy or not, regardless of the definition of STEMI/NSTEMI). In other words, millimeters really don't matter! hours duration.
She had this ECG recorded: Obvious massive anterior STEMI She was quickly brought to the critical care area and the cath lab was activated. Here is the ECG at 25 minutes: Terrible LAD STEMI (+) OMI So a CT scan was done which of course showed a normal aorta. This time the Queen of Hearts interpreted: No STEMI or Equivalent.
This ECG was recorded: It is difficult to appreciate P-waves, but I believe this is sinus tachycardia. It is correct that he did not have chest pain, but we must remember that fully 1/3 of full blown STEMI do not present with chest pain. This is extremely elevated for a type 2 MI and totally consistent with STEMI.
Smith comment: Approximately 33% of cases that everyone would call STEMI reperfuse spontaneously (TIMI-1, 2, 3 flow) before they undergo emergent angiogram (usually under 90 minute door to balloon time) 20% have TIMI-3 flow. The outcome in today's case was good but that was not due to expert ECG interpretation but rather a bit of luck.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


























Let's personalize your content