This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Written by Jesse McLaren A 70 year old with prior MIs and stents to LAD and RCA presented to the emergency department with 2 weeks of increasing exertional chest pain radiating to the left arm, associated with nausea. I sent this to the Queen of Hearts So the ECG is both STEMI negative and has no subtle diagnostic signs of occlusion.
Old ‘NSTEMI’ A history of coronary artery disease and a stent to the same territory further increases pre-test likelihood of acute coronary occlusion, including in-stent thrombosis. The patient had a history of ‘NSTEMI’ a decade prior, with an RCA stent. So this NSTEMI was likely a STEMI(-)OMI with delayed reperfusion.
While STEMI negative, the ECG is diagnostic of proximal LAD occlusion. Transient STEMI” are often managed like non-STEMI with delayed angiography, which is very risky. Cath lab was activated, and found a 95% proximal LAD occlusion which was stented. It’s unclear if the paramedic ECGs were seen or missed in the ED.
Nature Reviews Cardiology, Published online: 02 April 2024; doi:10.1038/s41569-024-01020-2 In ST-segment elevation myocardial infarction, the role of interventional modification of thrombi in the coronary arteries before stenting is controversial.
Subtle as a STEMI." (i.e., She was taken to the cath lab, where she was found to have 100% in-stent restenosis of the proximal LAD. In our study, there were 20/53 complete LAD OMI (TIMI-0 flow) which did not meet STEMI criteria. None of the 20 ever evolved to STEMI criteria. This one is easy for the Queen.
A prehospital “STEMI” activation was called on a 75 year old male ( Patient 1 ) with a history of hyperlipidemia and LAD and Cx OMI with stent placement. The two cases were considered: Patient 1 was recognized by the ED provider and the cardiologist as having resolved “STEMI”. It was stented. This was a large OMI.
This ECG is highly concerning for LAD occlusion despite it not showing a STEMI criteria. You can find the variables used to calculate the value on MD calc here: [link] Utilizing Dr. Smith’s Subtle Anterior STEMI Calculator (4-Variable), the value is greater than 18.2 The culprit mid LAD lesion was stented.
Now it is a full blown STEMI of 3 myocardial territories: inferior, posterior, and lateral But at least it does not call it "Normal." Successful drug-eluting stent placement opening up 95% mid RCA stenosis to 0% residual Nonobstructive left system disease. At this point — a STEMI was diagnosed, and cardiac cath with PCI was performed.
Patient still not having chest pain however this is more concerning for OMI/STEMI. Wellens' syndrome is a syndrome of Transient OMI (old terminology would be transient STEMI). As far as I can tell, there is only one randomized trial of immediate vs. delayed intervention for transient STEMI. Labs ordered but not yet drawn.
This is documented as a STEMI in the clinical notes and in the cath report, but certainly does not meet STEMI criteria and is therefore an NSTEMI by definition. For national registry purposes, this will be incorrectly classified as a STEMI.) Most STEMI have peak cTnI greater than 10.0. Large STEMI are approximately 30-80.
The cath lab was activated, and then not cancelled, and the angiogram showed 99% TIMI 2 flow proximal LAD culprit lesion, stented in less than 90 minutes of arrival. Cath days later showed complete occlusion of the LAD, stented. Another missed OMI by the False STEMI-NonSTEMI Dichotomy Don't miss them!!! Normal vitals.
Circulation, Volume 150, Issue Suppl_1 , Page A4132742-A4132742, November 12, 2024. A random-effects model was used for outcomes with high heterogeneity.Results:We included 4 RCTs with 3173 patients comparing FFR-guided CR with culprit-only PCI in patients with STEMI and multivessel coronary artery diseases.
Intra-procedural data included access route, coronary anatomy, lesion complexity, number of stents deployed, door-to-balloon time for primary PCI, and any intra-procedural complications. and the average number of stents 2.6. The radial approach was used in 544/567 (95.94%), the average SYNTAX score was 34.8 ± 9.6,
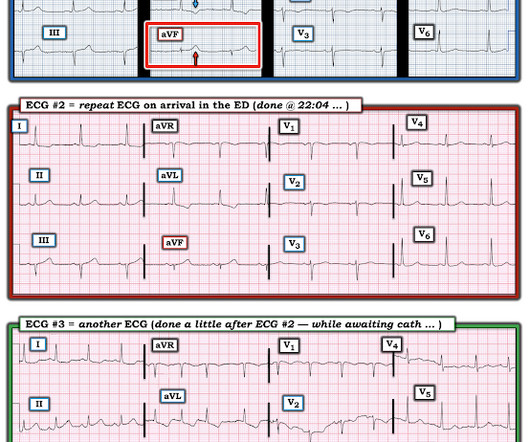
Another ECG was recorded while awaiting the cath team: Now there is STEMI Let's look at that first (prehospital ECG) again: Very subtle! It was opened and stented. I wondered the next day what the Queen would have said: OMI with high confidence!! Peak trop was 7000 ng/L (since the intervention was so fast)!!
On the combined basis of angiography and IVUS, this patient received stents to his mid RCA, proximal PDA, and OM. RCA and PDA before and after, arrows indicating stented regions. OM before and after, arrow indicating stented region. Reperfusion findings may not manifest obviously and immediately.
P.S.: Cardiac cath was performed — and showed a distal LA D "culprit" lesion that was successfully stented. It may look identical t o the ST-T wave appearance seen after a STEMI with marked troponin elevation, that has now reperfused ( be this reperfusion spontaneous — or by treatment with PCI or thrombolytics ).
Unfortunately, the cardiologist waited until the next day to refer the patient for angiography and intervention because patient did not meet criteria for "STEMI"." Successful primary angioplasty of the mid-circumflex artery towards the main marginal branch with the implantation of a drug-eluting stent. Good angiographic result.
The door to balloon time was incredibly short and there was a 100% circumflex occlusion that was opened and stented. The Non-STEMI, which was an OMI, was diagnosed much faster with AI on the ECG than with troponin. For more on ECG findings in pulmonary disease — Check out My Comment in the May 31, 2024 post in Dr. Smith's ECG Blog ).
Circulation, Volume 150, Issue Suppl_1 , Page A4125093-A4125093, November 12, 2024. Types of ACS include stable angina 5.3% (n=8), unstable angina 24% (n=36), NSTEMI 28.7% (n=43), and STEMI 24% (n=36). All patients had interventional PCI with balloon and stent insertion. The mean age of patients was 57.68 (SD= 11.19) years.
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chest pain relieved by rest. The Queen of Hearts AI app will hopefully be FDA approved in Q1 of 2024. An Impella was placed for cardiac output augmentation.
It definitely does not fulfill STEMI criteria, and I would argue that it would not lead to cath lab activation in most centers. As a result, this 45-year old man did not experince any delay in treatment — and a large diagonal branch of the LAD was stented with good outcome. To the uninitiated — this ECG may appear normal.
At 2111, the troponin I peaked at 12.252 ng/mL (this is in the range of STEMI patients, quite high). RAO Caudal View Post PCI This is the RAO Caudal view after thrombectomy and stent placement. At 1605, another repeat troponin resulted at 5.271 ng/mL. RAO Caudal view: This is the RAO Caudal view. The proximal LAD is now widely patent.
The is very small STE in III and aVF which do not meet STEMI criteria, hyperacute T waves, reciprocal TWI in aVL, and maximal STD in V2-V3 showing posterior OMI. The cath lab was activated despite lack of STEMI criteria, around 2 am in the morning. 33% of STEMI are reperfused by the time of angiography. Very frustrating.
But it does not meet the ridiculous "STEMI criteria" since there is not 1 mm of STE in any lead. Here is the circumflex after stenting: Wide open The cardiologist called Dr. Lufkin back and said "Great call!!" So this is acute OMI. What does the Queen of Hearts say? (Dr. Working in a smaller emergency facility — Dr.
The PMCardio Queen of Hearts app asks you, before giving an interpretation of OMI ("STEMI-Equivalent"), whether the patient's clinical presentation is high risk for OMI. In the November 27, 2024 post Drs. Dizziness is so unlikely to be OMI without an obvious ECG, that I am going to pretend that this patient presented with chest pain.
This ECG pattern is my favorite example of how the STEMI criteria are fundamentally flawed. At cath there was a 100% proximal LAD occlusion, which was opened and stented. We have a series of 20 TIMI-0 LAD Occlusions that do meet STEMI criteria. 2024, January 31). There is a de Winter T- wave pattern also in lead I.
The first EKG was concerning for a Wellen’s-like pattern of subtle reperfusion changes in the setting of stuttering anginal-equivalent symptoms, but none were diagnostic of STEMI or OMI. Later in the night, the patient became bradycardic and developed a Mobitz II pattern , but he remained asymptomatic and hemodynamically stable.
The CAG showed a 99% thrombotic lesion of the proximal RCA, which was stented. Smith comment: Approximately 33% of cases that everyone would call STEMI reperfuse spontaneously (TIMI-1, 2, 3 flow) before they undergo emergent angiogram (usually under 90 minute door to balloon time) 20% have TIMI-3 flow. scratching? )
It is diagnostic of OMI, but this is SUBACUTE OMI I sent this ECG to my "EKG Nerdz" friends, without any clinical info at all and they answered "OMI" The Queen said: "STEMI-Equivalent with High Confidence:" Notice she sees findings in both normal beats and PVCs. It was opened and stented. There are new Q-waves in aVL, V5-6.
The report describes heavy plaque in the proximal RCA by IVUS, but no lesions in the previously occluded RPL branch and no stent was deployed. Her ECG afterward is shown below: ECG from five days prior Smith : this shows an old inferior MI with persistent ST elevation. It is consistent with an inferior LV aneurysm.
At cath later the same day, a proximal 99% RCA culprit lesion was stented. Following the improvement in the ECG the patient's pain too improved drastically. This of course proves that the initial ECG was OMI and that the artery has reperfused. Troponin T peaked at 4051 ng/L. The difference is only 30 degrees and up to 45 degrees is normal.
The cath lab was deactivated by cardiologist on arrival at ED because it was "not a STEMI". First obtuse marginal also had an 80% stenosis and was stented. 2022;Available from: [link] Click here to sign up for Queen of Hearts Access. == MY Comment, by K EN G RAUER, MD ( 10/27/2024 ): == I view today's case as unfortunate.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





































Let's personalize your content