This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
ECG Blog #193 — Reviews the basics for predicting the " culprit " artery ( as well as reviewing why the term "STEMI" — should be replaced by "OMI" = O cclusion-based MI ). . = R elated E CG B log P osts to Today’s Case : ECG Blog #205 — Reviews my S ystematic A pproach to 12-lead ECG Interpretation.
3) We do not show the upward concavity measurement technique here. == MY Comment , by K EN G RAUER, MD ( 11/27 /2024 ): == For optimally time-efficient identification of acute OMI in the absence of frank ST elevation — it's essential to get good at recognizing hyperacute T waves. "A A picture is worth 1,000 words".
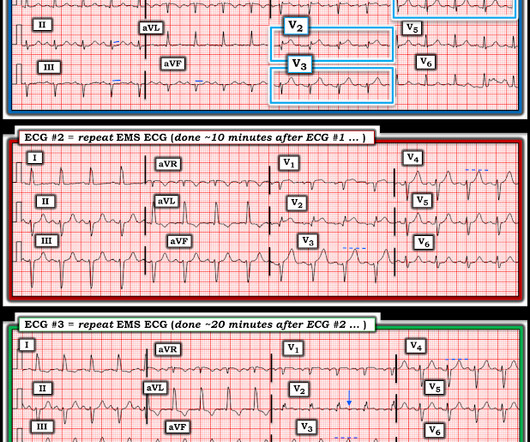
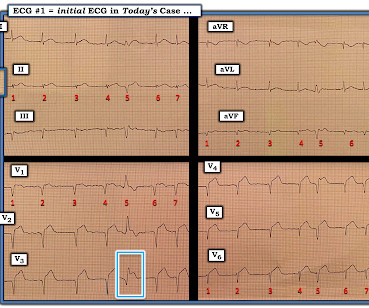
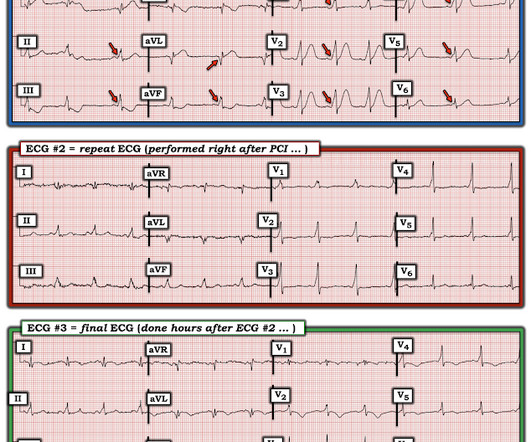
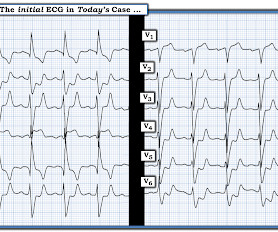
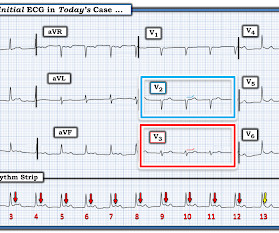
Interpretation : diagnostic of acute anterior OMI with STE less than STEMI criteria in V1-V4, hyperacute T waves in V2-V4, and suspiciously flat isoelectric ST segments in III and aVF suspicious for reciprocal findings. Now it even meets STEMI criteria, and HATWs continue to inflate. So the cath lab was not activated. Ongoing OMI.
So while there’s no diagnostic STEMI criteria, there are multiple ischemic abnormalities in 11/12 leads involving QRS, ST and T waves, which are diagnostic of a proximal LAD occlusion. First trop was 7,000ng/L (normal 25% of ‘Non-STEMI’ patients with delayed angiography have the exact same pathology of acute coronary occlusion.
Despite anticipation by many that the initial post-resuscitation ECG will show an obvious acute infarction — this expected "STEMI picture" is often not seen.
The ECG did not meet STEMI criteria, and the final cardiology interpretation was “ST and T wave abnormality, consider anterior ischemia”. There’s only minimal ST elevation in III, which does not meet STEMI criteria of 1mm in two contiguous leads. But STEMI criteria is only 43% sensitive for OMI.[1]
Obvious infero-postero-lateral STEMI(+)OMI, regardless of context Now let’s put them in order: what was the sequence? With serial ECGs that are ‘STEMI negative’ the physician could have waited for serial troponin levels or referred the patient as “non-STEMI”. What was the outcome and final diagnosis?
I sent this to the Queen of Hearts So the ECG is both STEMI negative and has no subtle diagnostic signs of occlusion. Non-STEMI guidelines call for “urgent/immediate invasive strategy is indicated in patients with NSTE-ACS who have refractory angina or hemodynamic or electrical instability,” regardless of ECG findings.[1]
tim.hodson Mon, 10/07/2024 - 14:45 Oct. 7, 2024 — The Society for Cardiovascular Angiography & Interventions (SCAI) recently announced the publication of the Expert Consensus Statement on the Management of Patients with STEMI Referred for Primary PCI.
The use of physiology-guided complete revascularization is superior to a culprit-only strategy for older patients with either STEMI or NSTEMI, according to a prespecified substudy of the FIRE trial presented at ESC Congress 2024 in London and simultaneously published in JACC.
Immediate Microvascular Physiology After Mechanical Coronary Reperfusion of STEMI. 2024 May, 83 (21) 2077–2079. 2024 May, 83 (21) 2066–2076. MRR = (CFR/FFR) × (P a,rest /P a,hyper ) References Michel Zeitouni, Ghilas Rahoual, Gilles Montalescot, and the ACTION study group. J Am Coll Cardiol. van Leeuwen, Stephen P. Zimmermann.
Circulation, Volume 150, Issue Suppl_1 , Page A4142231-A4142231, November 12, 2024. Background:Little is known about the clinical relevance of interleukin (IL)-6 and the severity of patients with acute ST-elevation myocardial infarction (STEMI). All information about clinical and paraclinical parameters was recorded.
The Minneapolis Heart Institute Foundation (MHIF) is presenting leading research focused on trends in ST-elevation myocardial infarction (STEMI), the most severe form of a heart attack, at the American College of Cardiology’s Annual Scientific Session (ACC.24), 24), being held April 6-8 in Atltanta, GA.
Nature Reviews Cardiology, Published online: 23 April 2024; doi:10.1038/s41569-024-01035-9 Data from the DanGer Shock trial demonstrate that implantation of a microaxial flow pump in patients with ST-segment elevation myocardial infarction complicated by cardiogenic shock increases the survival rate compared with standard care alone.
So this NSTEMI was likely a STEMI(-)OMI with delayed reperfusion. The patient was admitted as ‘NSTEMI’ which is supposed to represent a non-occlusive MI, but the underlying pathophysiology is analogous to a transient STEMI. West J Emerg Med 2024). Fortunately the patient did not reocclude while awaiting the angiogram.
While STEMI negative, the ECG is diagnostic of proximal LAD occlusion. Transient STEMI” are often managed like non-STEMI with delayed angiography, which is very risky. This case is an example of the steps we can all take in daily practice as the paradigm shifts from STEMI to OMI.
This certainly looks like an anterior STEMI (proximal LAD occlusion), with STE and hyperacute T-waves (HATW) in V2-V6 and I and aVL. How do you explain the anterior STEMI(+)OMI immediately after ROSC evolving into posterior OMI 30 minutes later? This caused a type 2 anterior STEMI.
If we took this as the gold standard, we would conclude that the computer interpretation was safe and accurate at least accurate enough to not miss STEMI, and that physicians should not be interrupted to interpret it, because there would be no change in patient management. What is the gold standard for ECG interpretation: patient outcome!!!
Circulation, Volume 150, Issue Suppl_1 , Page A4147134-A4147134, November 12, 2024. Introduction:Elevated LDL cholesterol is linked to microvascular injury and adverse cardiac events in STEMI patients. This study examines the impact of prior statin use on LDL levels at the time of MI, focusing on NSTEMI and STEMI patients.
IMPRESSION: In this patient who presents with severe, new-onset CP — today's ECG is diagnostic of an extensive, ongoing antero-lateral STEMI. ECG Blog #193 — Reviews the basics for predicting the " culprit " artery ( as well as reviewing why the term "STEMI" — should be replaced by "OMI" = O cclusion-based MI ).
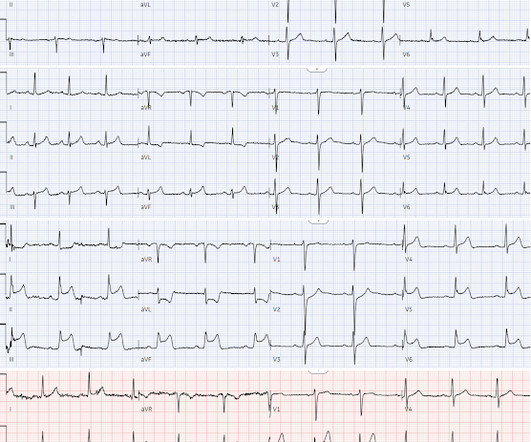
Its hard to measure the STE in I exactly with the moving baseline, but there is almost certainly not enough STE to meet STEMI criteria. The ACC recognizes these findings as formal STEMI equivalents (though they do not define how to find them). They are symmetric, fat, convex on both sides, etc. 13 post.
Prompt cath is therefore advised if the post-ROSC shows an acute STEMI. To Emphasize: The phenomenon of T-QRS-D is not needed in today's case to recognize the acute STEMI. The decision of whether to cath patients with a less definitive post-ROSC ECG is less clear.
This was a machine read STEMI positive OMI. The meaning of this quote is that at times, something as obvious as the dramatic anterior lead ST elevation that we see in today's tracing is not the result of an acute LAD STEMI. His ECG is shown below. Pretty obvious anterior current of injury. What would you guess is the culprit artery?
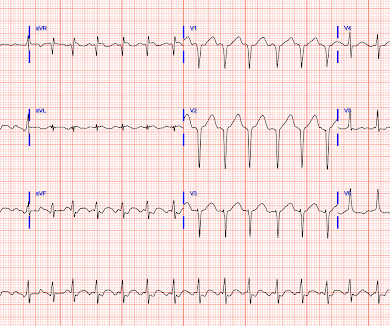
Written by Bobby Nicholson What do you think of this “STEMI”? Second, although there is a lot of ST Elevation which meets STEMI criteria, especially in V3-4, the ST segment is extremely upwardly concave with very large J-waves (J-point notching). With EMS, patient had a GCS of 3 and was saturating 60% on room air. ng/mL and 0.10
Nature Reviews Cardiology, Published online: 02 April 2024; doi:10.1038/s41569-024-01020-2 In ST-segment elevation myocardial infarction, the role of interventional modification of thrombi in the coronary arteries before stenting is controversial.
Publication date: Available online 21 March 2024 Source: The American Journal of Cardiology Author(s): Dániel Tornyos, Réka Lukács, András Jánosi, András Komócsi
My New E CG P odcasts ( 5/28/2024 ): These podcasts are part of the Mayo Clinic Cardiovascular CME Podcasts Series ( "Making Waves" ) — hosted by Dr. Anthony Kashou. 2:00 — Dr. Kashou to Dr. Grauer: "In 2024 — Where do you see computerized ECG interpretations and AI?" How much "human oversight" is needed?
Publication date: Available online 2 July 2024 Source: The American Journal of Cardiology Author(s): Sara J. King, Rajiv Patel, Sameer Arora, George A.
Subtle as a STEMI." (i.e., Here is the bottom line of the article: It is widely believed that hyperacute T-waves are a transitional state preceding ST Elevation 1–4 Thus, it is tempting to postulate that early cases of OMI will eventually evolve to STEMI; yet, our data contradicts that notion. This one is easy for the Queen.
Now it is a full blown STEMI of 3 myocardial territories: inferior, posterior, and lateral But at least it does not call it "Normal." Learning Points: You cannot trust conventional algorithms even to find STEMI(+) OMI, even when they say "normal ECG." At this point — a STEMI was diagnosed, and cardiac cath with PCI was performed.
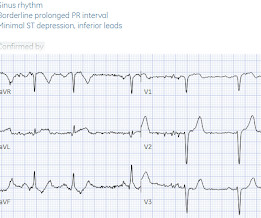
The prehospital and ED computer interpretation was inferior STEMI: There’s normal sinus rhythm, first degree AV block and RBBB, normal axis and normal voltages. The paramedic notes called STEMI into question: “EMS disagree with monitor for STEMI callout. Vitals were normal except for oxygen saturation of 94%. Vitals were normal.
Publication date: Available online 22 December 2024 Source: The American Journal of Cardiology Author(s): Sahib Singh, Udaya S Tantry, Young-Hoon Jeong, Paul A Gurbel
A prehospital “STEMI” activation was called on a 75 year old male ( Patient 1 ) with a history of hyperlipidemia and LAD and Cx OMI with stent placement. The two cases were considered: Patient 1 was recognized by the ED provider and the cardiologist as having resolved “STEMI”. He wrote most of it and I (Smith) edited.
ECG Blog #193 — Reviews the basics for predicting the " culprit " artery ( as well as reviewing why the term "STEMI" — should be replaced by "OMI" = O cclusion-based MI ). R elated E CG B log P osts to Today’s Case : ECG Blog #205 — Reviews my S ystematic A pproach to 12-lead ECG Interpretation.
Publication date: Available online 14 November 2024 Source: The American Journal of Cardiology Author(s): Aiham Albaeni, Shuang Li, Yong Shan, Ravi Thakker, Diann E. Gaalema, Ritika Saxena MPH, Yong-fang Kuo, Hani Jneid, James Goodwin
Publication date: Available online 3 January 2024 Source: The American Journal of Cardiology Author(s): Amine Bouchlarhem, Salma Bouyadid, Zakaria Bazid, Nabila ismaili, Noha El ouafi
The conventional machine algorithm interpreted this ECG as STEMI. See this post of RV MI with both McConnell sign and "D" sign: Inferior and Posterior STEMI. I've excerpted the Table shown below in Figure-2 from My Comment in that June 17, 2024 post. When EMS found her, she was dyspneic and diaphoretic.
ECG Blog #193 — Reviews the basics for predicting the " culprit " artery ( as well as reviewing why the term "STEMI" — should be replaced by "OMI" = O cclusion-based MI ). . = R elated E CG B log P osts to Today’s Case : ECG Blog #205 — Reviews my S ystematic A pproach to 12-lead ECG Interpretation.
This is documented as a STEMI in the clinical notes and in the cath report, but certainly does not meet STEMI criteria and is therefore an NSTEMI by definition. For national registry purposes, this will be incorrectly classified as a STEMI.) Most STEMI have peak cTnI greater than 10.0. Large STEMI are approximately 30-80.
The benefits of complete revascularization over culprit-only coronary artery revascularization were confirmed in older patients with ST-segment elevation myocardial infarction (STEMI) and multivessel disease over the first 4 years, according to late-breaking research presented in a Hot Line session today at ESC Congress 2024.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.







































Let's personalize your content