This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
The ECG did not meet STEMI criteria, and the final cardiology interpretation was “ST and T wave abnormality, consider anterior ischemia”. There’s only minimal ST elevation in III, which does not meet STEMI criteria of 1mm in two contiguous leads. But STEMI criteria is only 43% sensitive for OMI.[1]
The benefits of complete revascularization over culprit-only coronary artery revascularization were confirmed in older patients with ST-segment elevation myocardialinfarction (STEMI) and multivessel disease over the first 4 years, according to late-breaking research presented in a Hot Line session today at ESC Congress 2024.
I sent this to the Queen of Hearts So the ECG is both STEMI negative and has no subtle diagnostic signs of occlusion. Non-STEMI guidelines call for “urgent/immediate invasive strategy is indicated in patients with NSTE-ACS who have refractory angina or hemodynamic or electrical instability,” regardless of ECG findings.[1]
Nature Reviews Cardiology, Published online: 23 April 2024; doi:10.1038/s41569-024-01035-9 Data from the DanGer Shock trial demonstrate that implantation of a microaxial flow pump in patients with ST-segment elevation myocardialinfarction complicated by cardiogenic shock increases the survival rate compared with standard care alone.
It is now well known that even if a coronary artery is opened well after a myocardialinfarction, with good flow in the epicardial coronary arteries, there could be impaired myocardial perfusion. Immediate Microvascular Physiology After Mechanical Coronary Reperfusion of STEMI. 2024 May, 83 (21) 2077–2079.
The Minneapolis Heart Institute Foundation (MHIF) is presenting leading research focused on trends in ST-elevation myocardialinfarction (STEMI), the most severe form of a heart attack, at the American College of Cardiology’s Annual Scientific Session (ACC.24), 24), being held April 6-8 in Atltanta, GA.
Subtle as a STEMI." (i.e., Here is the bottom line of the article: It is widely believed that hyperacute T-waves are a transitional state preceding ST Elevation 1–4 Thus, it is tempting to postulate that early cases of OMI will eventually evolve to STEMI; yet, our data contradicts that notion. This one is easy for the Queen.
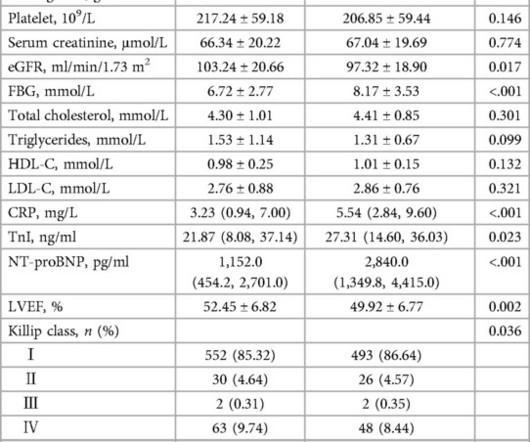
Circulation, Volume 150, Issue Suppl_1 , Page A4142231-A4142231, November 12, 2024. Background:Little is known about the clinical relevance of interleukin (IL)-6 and the severity of patients with acute ST-elevation myocardialinfarction (STEMI). All information about clinical and paraclinical parameters was recorded.
This is a value typical for a large subacute MI, n ormal value 48 hours after myocardialinfarction is associated with Post-Infarction Regional Pericarditis ( PIRP ). Mechanical complications secondary to myocardialinfarction are infrequent due to most patients receiving revascularization quite rapidly.
Here is his ED ECG at triage: Obvious high lateral OMI that does not quite meet STEMI criteria. Thus, it has recently become generally accepted that most plaque ruptures resulting in myocardialinfarction occur in plaques that narrow the lumen diameter by 40% of the arterial cross section may be involved by plaque.
Nature Reviews Cardiology, Published online: 02 April 2024; doi:10.1038/s41569-024-01020-2 In ST-segment elevation myocardialinfarction, the role of interventional modification of thrombi in the coronary arteries before stenting is controversial.
Circulation, Volume 150, Issue Suppl_1 , Page A4147134-A4147134, November 12, 2024. Introduction:Elevated LDL cholesterol is linked to microvascular injury and adverse cardiac events in STEMI patients. This study examines the impact of prior statin use on LDL levels at the time of MI, focusing on NSTEMI and STEMI patients.
Patient still not having chest pain however this is more concerning for OMI/STEMI. Wellens' syndrome is a syndrome of Transient OMI (old terminology would be transient STEMI). A comparison of electrocardiographic changes during reperfusion of acute myocardialinfarction by thrombolysis or percutaneous transluminal coronary angioplasty.
Written by Bobby Nicholson What do you think of this “STEMI”? Second, although there is a lot of ST Elevation which meets STEMI criteria, especially in V3-4, the ST segment is extremely upwardly concave with very large J-waves (J-point notching). With EMS, patient had a GCS of 3 and was saturating 60% on room air. ng/mL and 0.10
Smith : there is some minimal ST elevation in V2-V6, but does not meet STEMI criteria. Transient STEMI has been studied and many of these patients will re-occlude in the middle of the night. Timing of revascularization in patients with transient ST segment elevation myocardialinfarction: a randomized clinical trial.
“ Since Intravenous lysis looks too simplistic, that do not need expertise, and lacks a commercial trail, it is wrongly depicted as inferior management strategy in STEMI “ Every one of us is equally responsible for this sorry state of affairs. In LAD STEMI time is more crucial. NRMI data Ref 2) 2.There
What we can do, at our level is to incorporate a new term “ benign or micro myocardialInfarction” – akin to lacunar infarcts or TIA equivalents of the brain in the heart. Is MyocardialInfarction Overdiagnosed? Published online April 24, 2024. Reference 1.McCarthy doi:10.1001/jama.2024.5235
Circulation, Volume 150, Issue Suppl_1 , Page A4141279-A4141279, November 12, 2024. Background:Slow flow phenomenon is impaired coronary flow during percutaneous coronary intervention (PCI) in absence of mechanical obstruction, and it is associated with deteriorated outcome.
The emergency physician asked the advice of Dr. Reiters because of absence of STEMI criteria. Translation from French: Acute Occlusion MyocardialInfarction with High Confidence. But if the pain is persistent, as reported, then the patient must go to the cath lab even if the ECG suggests reperfusion.
Clinical presentation was stable angina 130/567 (22.9%), non-ST-elevation acute coronary syndrome (NSTEACS) 312/567 (55%), ST-elevation myocardialinfarction (STEMI) 125/567 (22.0%), and STEMI with cardiogenic shock 13/125 (10.4%). The radial approach was used in 544/567 (95.94%), the average SYNTAX score was 34.8 ± 9.6,
The ECG is diagnostic of occlusion myocardialinfarction (OMI). It definitely does not fulfill STEMI criteria, and I would argue that it would not lead to cath lab activation in most centers. The overall read is OMI with HIGH confidence. == Below is the ECG of Patient #2 — as interpreted by the QOH.
The ECG was read as "No STEMI" and the patient was treated like an average chest pain patient (despite the fact that a chest pain patient with active pain and active subendocardial ischemia is very high risk). The Queen of Hearts AI app will hopefully be FDA approved in Q1 of 2024. It is already approved in Europe. Eur J Emerg Med.
So there is probability of myocardial injury here (and because it is in the correct clinical setting, then myocardialinfarction.) Sometimes it can take 12 or 24 hours to see ECG evidence of reperfusion. == MY Comment , by K EN G RAUER, MD ( 1/4/ 2024 ): == Superb and thorough discussion by Dr. Frick of today's case!
The limb leads have been removed because there was no ST elevation in those leads, the QRS complexes have been obscured because this is irrelevant to STEMI criteria, and red lines have been added to measure ST segment elevation. But STEMI criteria ignore all this and look at ST segments in isolation.
Circulation, Volume 150, Issue Suppl_1 , Page A4141170-A4141170, November 12, 2024. In cardiovascular research, serotonin has been implicated in modulating vascular tone, platelet aggregation, and myocardial function. Conclusion:Higher 5-HTP levels are independently associated with a reduced risk of MACE in patients after STEMI.
The receiving emergency physician consulted with interventional cardiology who stated there was no STEMI. AIVR is not always the result of significant pathology, but is classically associated with the reperfusion phase of acute myocardialinfarction. Is there STEMI? The patient continued having chest pain. Moffat, M.
Patients with ST-segment elevation myocardialinfarction (STEMI) and complex coronary artery disease (CAD) face a poor prognosis, including increased heart failure (HF) risk. We performed a pooled secondary analysis of 139 patients with STEMI. We performed a pooled secondary analysis of 139 patients with STEMI.
Circulation: Cardiovascular Imaging, Volume 17, Issue 12 , Page e017041, December 1, 2024. BACKGROUND:The presence and clinical significance of hepatic tissue alterations as assessed by cardiac magnetic resonance imaging in patients with ST-segmentelevation myocardialinfarction (STEMI), are unclear.
Circulation, Volume 150, Issue Suppl_1 , Page A4132742-A4132742, November 12, 2024. A random-effects model was used for outcomes with high heterogeneity.Results:We included 4 RCTs with 3173 patients comparing FFR-guided CR with culprit-only PCI in patients with STEMI and multivessel coronary artery diseases.
An invasive treatment strategy involving coronary angiography and revascularization plus medical therapy did not significantly lower the composite risk of cardiovascular death or nonfatal myocardialinfarction (MI) compared with a conservative strategy of medical therapy alone in older adults with NSTEMI, according to findings from the SENIOR-RITA (..)
It was read by the treating physician and the overreading cardiologist as "Paced, no STEMI." Immediate and early percutaneous coronary intervention in very high risk and high risk non-ST segment elevation myocardialinfarction patients. How does the Queen of Hearts do? Ann Emerg Med [Internet]. 2012;60:766–776. 2023;131569.
In this study, we investigated the safety and efficacy of fondaparinux sodium in post-percutaneous coronary intervention (PCI) anticoagulation therapy for patients with ST-segment elevation myocardialinfarction. There are a total of 200 patients with ST segment elevation myocardialinfarction underwent PCI and anticoagulation therapy.
Unfortunately, the cardiologist waited until the next day to refer the patient for angiography and intervention because patient did not meet criteria for "STEMI"." This is an enormous posterior infarct! And Olivier finishes with this commentary: "Yet another example in favor of abandoning STEMI criteria for diagnosing OMI.
The ECG shows obvious STEMI(+) OMI due to probable proximal LAD occlusion. Troponin T peaked at 38,398 ng/L ( = a very large myocardialinfarction, but not massive-- thanks to the pre-PCI spontaneous reperfusion, and rapid internvention!! ). The below ECG was recorded. Inotropic medication was continued.
milla1cf Mon, 04/08/2024 - 18:07 April 8, 2024 — Implantation of the Impella CP micro-axial flow pump in the hours after a heart attack significantly increased the rate of survival at six months among people suffering cardiogenic shock, according to a study presented at the American College of Cardiology ’s Annual Scientific Session.
Circulation, Volume 150, Issue Suppl_1 , Page A4137939-A4137939, November 12, 2024. However, little is known about LOY and prognosis of ST-segment elevation myocardialinfarction (STEMI).Hypothesis:We However, little is known about LOY and prognosis of ST-segment elevation myocardialinfarction (STEMI).Hypothesis:We
BackgroundContrast-induced acute kidney injury (CI-AKI) is a common complication in patients with ST-segment elevation myocardialinfarction (STEMI) and is associated with an inflammatory response. Integrating IBI can improve the risk stratification of STEMI patients regarding CI-AKI.
of patients with anterior myocardialinfarction ( 1 ). This ECG pattern is my favorite example of how the STEMI criteria are fundamentally flawed. We have a series of 20 TIMI-0 LAD Occlusions that do meet STEMI criteria. Tall precordial T waves with depressed ST take-off: an early sign of acute myocardialinfarction?
She had this ECG recorded: Obvious massive anterior STEMI She was quickly brought to the critical care area and the cath lab was activated. Here is the ECG at 25 minutes: Terrible LAD STEMI (+) OMI So a CT scan was done which of course showed a normal aorta. This time the Queen of Hearts interpreted: No STEMI or Equivalent.
This OMI went unrecognized and, had the artery not re-perfused by itself, the patient could have suffered a very large myocardialinfarction. The Queen of Hearts AI model confidently identifies the first ECG in today's case as occlusion myocardialinfarction (OMI HIGH confidence). He was diagnosed with NSTEMI.
It is correct that he did not have chest pain, but we must remember that fully 1/3 of full blown STEMI do not present with chest pain. They made a final diagnosis of type II myocardialinfarction. This is extremely elevated for a type 2 MI and totally consistent with STEMI. The EKG shows inferior OMI.
It is diagnostic of OMI, but this is SUBACUTE OMI I sent this ECG to my "EKG Nerdz" friends, without any clinical info at all and they answered "OMI" The Queen said: "STEMI-Equivalent with High Confidence:" Notice she sees findings in both normal beats and PVCs. The November 8, 2024 post — artifact complicating OMI assessment.
All of these findings together makes this ECG diagnostic of inferior and posterior occlusion myocardialinfarction (OMI) The patient is this case was treated as if he had an ongoing OMI. When looking at the precordial leads there is appreciable slight ST depression in lead V2 and inappropriately isoelectric ST segment i lead V3.
The cath lab was deactivated by cardiologist on arrival at ED because it was "not a STEMI". Immediate and early percutaneous coronary intervention in very high-risk and high-risk non-ST segment elevation myocardialinfarction patients. Pt received 324 ASA and 2 sprays of nitro with improvement. Pain was decreased to 2/10.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.












































Let's personalize your content