This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Here is his ED ECG at triage: Obvious high lateral OMI that does not quite meet STEMI criteria. This confirms that the pain was ischemia and is now resovled. He does have a recently diagnosed PE, and has not been taking his anticoagulation due to cost. He was given aspirin and sublingual nitro and the pain resolved.
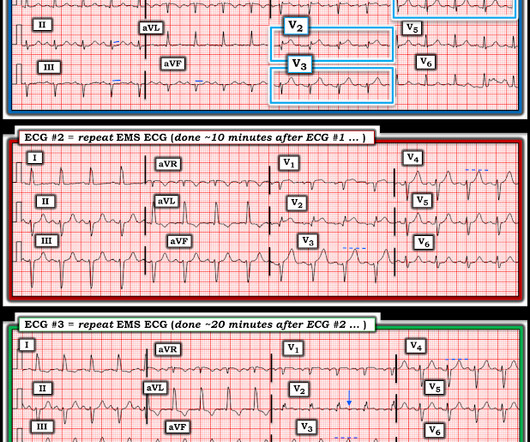
Interpretation : diagnostic of acute anterior OMI with STE less than STEMI criteria in V1-V4, hyperacute T waves in V2-V4, and suspiciously flat isoelectric ST segments in III and aVF suspicious for reciprocal findings. Now it even meets STEMI criteria, and HATWs continue to inflate. So the cath lab was not activated. Ongoing OMI.
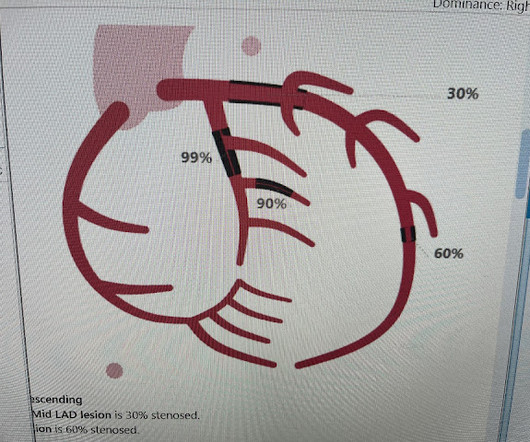
The ECG did not meet STEMI criteria, and the final cardiology interpretation was “ST and T wave abnormality, consider anterior ischemia”. There’s only minimal ST elevation in III, which does not meet STEMI criteria of 1mm in two contiguous leads. But STEMI criteria is only 43% sensitive for OMI.[1]
The ECG shows severe ischemia, possibly posterior OMI. But cardiac arrest is a period of near zero flow in the coronary arteries and causes SEVERE ischemia. It takes time for that ischemia to resolve. Cardiac arrest #3: ST depression, Is it STEMI? And what do you want to do?
I sent this to the Queen of Hearts So the ECG is both STEMI negative and has no subtle diagnostic signs of occlusion. Non-STEMI guidelines call for “urgent/immediate invasive strategy is indicated in patients with NSTE-ACS who have refractory angina or hemodynamic or electrical instability,” regardless of ECG findings.[1]
This certainly looks like an anterior STEMI (proximal LAD occlusion), with STE and hyperacute T-waves (HATW) in V2-V6 and I and aVL. This rules out subendocardial ischemia and is diagnostic of posterior OMI. How do you explain the anterior STEMI(+)OMI immediately after ROSC evolving into posterior OMI 30 minutes later?
This was a machine read STEMI positive OMI. In this patient's case, the RV ischemia manifested as dramatic anterior hyperacute T waves. This degree of STE is a bit atypical for LAD ischemia. Written by Willy Frick A 50 year old man with no medical history presented with acute onset substernal chest pain. His ECG is shown below.
Below is the first ECG recorded by paramedics after 2 hours of chest pain, interpreted by the machine as “possible inferior ischemia”. While STEMI negative, the ECG is diagnostic of proximal LAD occlusion. Transient STEMI” are often managed like non-STEMI with delayed angiography, which is very risky. What do you think?
Instead, pain is numbed and thus ischemia is obscured with opioids, excuses like hypertension are blamed, and unnecessary CT pulmonary angiograms are focused on. This patient does not show up in the STEMI registry, and the time to reperfusion will likely not be identified as the problem that it was. You will get 5 free reports.
Written by Bobby Nicholson What do you think of this “STEMI”? or basilar ischemia. Second, although there is a lot of ST Elevation which meets STEMI criteria, especially in V3-4, the ST segment is extremely upwardly concave with very large J-waves (J-point notching). EKG on arrival to the ED is shown below: What do you think?
The fact that R waves 2 through 6 are junctional does make ischemia more difficult to interpret -- but not impossible. Back to the assessment of ischemia: Returning to the ECG, the leads that catch my eye first are -- I, II, V4, V5, V6. For national registry purposes, this will be incorrectly classified as a STEMI.) < 0.049).
I thought this finding consistent with the finding of ST depression in lateral leads I; V4,V5,V6 — and possibly indicative of multivessel disease ( ie, Diffuse Subendocardial Ischemia — as discussed in ECG Blog #400 ). ECG Blog #400 — Reviews the concept of " dynamic " ST-T wave changes ( and also Diffuse Subendocardial Ischemia ).
A prehospital “STEMI” activation was called on a 75 year old male ( Patient 1 ) with a history of hyperlipidemia and LAD and Cx OMI with stent placement. Whether these EKGs show myocarditis, a normal variant, or something else, they are overall not typical of transmural ischemia of the anterior or high lateral walls.
The ECG shows obvious STEMI(+) OMI due to probable proximal LAD occlusion. There is no definite evidence of acute ischemia. (ie, Simply stated — t he patient was having recurrent PMVT without Q Tc prolongation, and without evidence of ongoing transmural ischemia. ( The below ECG was recorded.
In any case, the ECG is diagnostic of severe ischemia and probably OMI. So this could be myocarditis but in my opinion needs an angiogram before making that diagnosis. == Dr. Nossen Comment/Interpretation: Evaluation of ischemia on an ECG can be very challenging. Concordant STE of 1 mm in just one lead or 2a.
It has been estimated that in the aggregate, they occur at a rate of about 3 per 1000 patients with acute MI, and most of these events occur in patients with STEMI. A mong patients with STEMI, ventricular septal rupture is the most common and free wall rupture is the least common. Hammill SC. Edwards WD.
The baseline ECG is basically normal with no ischemia. You can see in the lead-specific analysis that she "sees" the STD in V5, V5, and II, with STE in aVR as signs of "Not OMI", because subendocardial ischemia pattern is not the same as OMI. In my opinion, I think it looks more like subendocardial ischemia.
The receiving emergency physician consulted with interventional cardiology who stated there was no STEMI. Is there STEMI? Possible mechanisms of ventricular arrhythmias elicited by ischemia followed by reperfusion. About one hour later his high sensitivity troponin I resulted at 3,000 ng/L (reference 3-54 ng/L). Moffat, M.
QOH versions 1 and 2 both say Not OMI, with high confidence, without any clinical context, despite the abnormal STE meeting STEMI criteria. The patient did well. == MY Comment , by K EN G RAUER, MD ( 8/4 /2024 ): == I thought today's case by Dr. Meyers is an important one for emergency providers for a number of reasons.
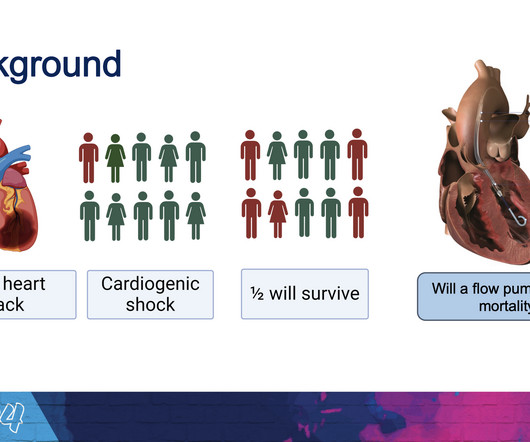
milla1cf Mon, 04/08/2024 - 18:07 April 8, 2024 — Implantation of the Impella CP micro-axial flow pump in the hours after a heart attack significantly increased the rate of survival at six months among people suffering cardiogenic shock, according to a study presented at the American College of Cardiology ’s Annual Scientific Session.
Another missed OMI by the False STEMI-NonSTEMI Dichotomy Don't miss them!!! In addition — there is transmural ischemia of the septum , most often resulting from occlusion proximal to the 1st septal perforator branch of the LAD. Stopped measuring troponins on the day of presentation around 5,000 ng/L as it was still rising."
At 2111, the troponin I peaked at 12.252 ng/mL (this is in the range of STEMI patients, quite high). The patient’s angiogram should have been expedited, but the EKG change was not recognized as recurrence of transmural ischemia. At 1605, another repeat troponin resulted at 5.271 ng/mL.
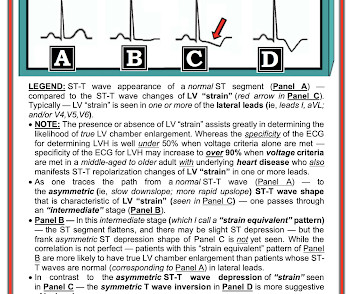
The ECG shows sinus rhythm with normal QRS complex morphology and significant subendocardial ischemia (SEI) pattern (ST depression in many leads, worst in lateral areas including leads II, V5-6, with reciprocal STE in aVR). Here is her ECG within 30 minutes of PCI: Improved, but still with ischemia. hours duration.
But it does not meet the ridiculous "STEMI criteria" since there is not 1 mm of STE in any lead. Learn to read the ECG for sublte OMI, and get the Queen of Hearts. == MY Comment , by K EN G RAUER, MD ( 11/1 /2024 ): == The beauty of today's case is its simple efficiency. So this is acute OMI. What does the Queen of Hearts say? (Dr.
Radionuclide scan was negative for ischemia. For cases similar to today, in which LVH may mimic ischemia Check out My Comment at the bottom of the page of the following posts in Dr. Smith's ECG Blog the November 29, 2023 post June 20, 2020 March 31, 2019 March 29, 2019 and t he December 27, 2018 post. Chest X-Ray was normal.
She had this ECG recorded: Obvious massive anterior STEMI She was quickly brought to the critical care area and the cath lab was activated. Here is the ECG at 25 minutes: Terrible LAD STEMI (+) OMI So a CT scan was done which of course showed a normal aorta. This time the Queen of Hearts interpreted: No STEMI or Equivalent.
This ECG pattern is my favorite example of how the STEMI criteria are fundamentally flawed. We have a series of 20 TIMI-0 LAD Occlusions that do meet STEMI criteria. However, many patients with de Winter ECG pattern have TIMI 0 at angiography and the ECG pattern does not necessarily progress to STEMI. 2024, January 31).
The Queen of Hearts Diagnosed "STEMI/STEMI equivalent" on that first ECG (she now uses "STEMI Equivalent" rather than OMI). The fact that she states "STEMI-Equivalent" here means that she does not think it is reperfused, but she does not know that the patient is pain free now. This is the new version of the Queen.
Smith : I recognize this as a STEMI mimic. Doesn't this necessarily mean that he was having ischemia? Here is his ECG: There is significant ST Elevation in inferior leads, with reciprocal ST depression in aVL. This appears to be an inferior OMI What do you think? I was not alarmed. What does the Queen of Hearts think? "No
The first EKG was concerning for a Wellen’s-like pattern of subtle reperfusion changes in the setting of stuttering anginal-equivalent symptoms, but none were diagnostic of STEMI or OMI. A good size infarct that no longer has active ischemia will have continually rising troponins due to the damage that was done hours ago.
Time 7 hours lead reversal There is limb lead reversal (QRS in I and aVL are now inverted), but nevertheless one can see that the ischemia appears to have resolved. Negative trops and negative angiogram does not rule out coronary ischemia or ACS. This is extremely elevated for a type 2 MI and totally consistent with STEMI.
50% of LAD STEMI have Q-waves by one hour. Smith : In limb leads, the ST vector is towards lead II (STE lead II STE lead III, which is more likely with pericarditis than with STEMI). There were no other causes of dyspnea apparent and thus we can assume that myocardial ischemia started 6 days prior. See Raitt et al.:
It is diagnostic of OMI, but this is SUBACUTE OMI I sent this ECG to my "EKG Nerdz" friends, without any clinical info at all and they answered "OMI" The Queen said: "STEMI-Equivalent with High Confidence:" Notice she sees findings in both normal beats and PVCs. The November 8, 2024 post — artifact complicating OMI assessment.
Ischemia often produces a straightening of the ST segment and sometimes upward convexity. Discussion: When a patient presents with chest pain and ST segment elevation we need to evaluate whether or not the ST elevation is ischemic in nature. iii ) An isolated Q wave in lead III ( as we see here ) — is not necessarily abnormal.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





































Let's personalize your content