This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Written by Jesse McLaren A healthy 75 year old developed 7/10 chestpain associated with diaphoresis and nausea, which began on exertion but persisted. Below is the first ECG recorded by paramedics after 2 hours of chestpain, interpreted by the machine as “possible inferior ischemia”. What do you think?
No ChestPain, but somnolent. The fact that this is syncope makes give it a far lower pretest probability than chestpain, but it was really more than syncope, as the patient actually underwent CPR and had hypotension on arrival of EMS. Former resident: "Just saw cath report, LAD stent was 100% acutely occluded."
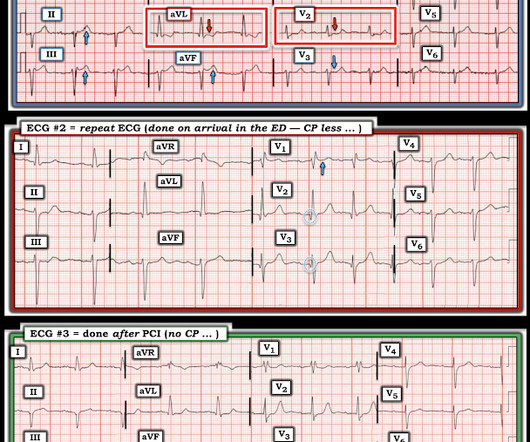
Written by Magnus Nossen with Edits by Grauer and Smith The ECGs in today’s case are from 3 different patients all presenting with new-onset CP ( ChestPain ). As a result, this 45-year old man did not experince any delay in treatment — and a large diagonal branch of the LAD was stented with good outcome.
A 50-something male with hypertension and 20- to 40-year smoking history presented with 1 week of stuttering chestpain that is worse with exertion, which takes many minutes to resolve after resting and never occurs at rest. At times the pain does go to his left neck. It is a ssociated with mild dyspnea on exertion.
I was working at triage when the medics brought this patient who is 65 yo and has had chestpain for 12 hours. It was opened and stented. Click here to sign up for Queen of Hearts Access == MY Comment , by K EN G RAUER, MD ( 7/20 /2024 ): == Today's case illustrates the importance of attention to subtle serial ECG findings.
Given the presentation, the cardiologist stented the vessel and the patient returned to the ICU for ongoing critical care. He did not remember whether he had experienced any chestpain. (TIMI 3 means the rate of passage of dye through the coronary artery is normal by angiography.) Two subsequent troponins were down trending.
Written by Willy Frick A man in his 50s with history of hypertension, hyperlipidemia, and a 30 pack-year smoking history presented to the ER with 1 hour of acute onset, severe chestpain and diaphoresis. His ECG is shown: What do you think? What do you think? This was the cost of preventing infarction of the anterior wall.)
Written by Jesse McLaren, comments by Smith A 55 year old with a history of NSTEMI presented with two hours of exertional chestpain, with normal vitals. Old ‘NSTEMI’ A history of coronary artery disease and a stent to the same territory further increases pre-test likelihood of acute coronary occlusion, including in-stent thrombosis.
TheNational Institute for Health and Care Excellence(NICE) recommends CCTA as the first-line investigation for patients with chestpain due to suspected CAD, highlighting its importance in improving diagnostic certainty. 2024,November 8). 2012) 380:2095128. 10.1016/S0140-6736(12)61728-0. link] iv IMV.2023 v Walter, M.
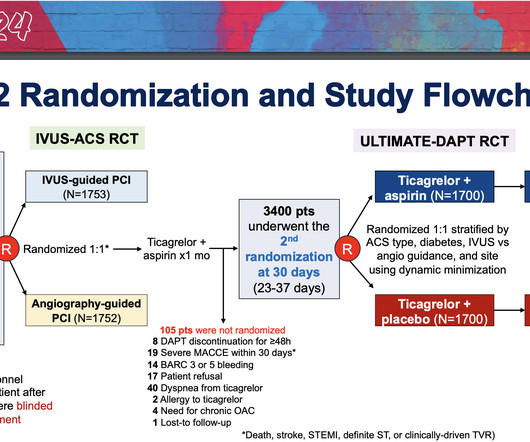
The study focused on patients who underwent PCI for acute coronary syndromes (ACS)—life-threatening conditions which include heart attacks and chestpain caused by decreased blood flow to the heart—with stents containing drugs to prevent further plaque buildup. Stents were supplied by Medtronic Corp. Minnesota, U.S.)
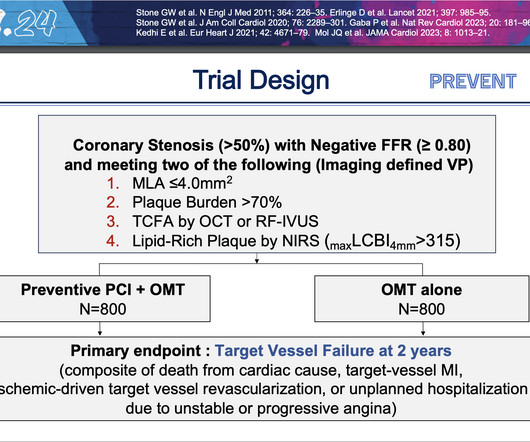
At two years, people who underwent preventive PCI were 89% less likely to experience the composite primary endpoint of cardiac death, heart attack in the target vessel, revascularization due to ischemia in the target vessel or hospitalization for unstable or progressive chestpain compared with people who received medications alone.
Circulation, Volume 150, Issue Suppl_1 , Page A4137144-A4137144, November 12, 2024. Introduction:Subacute stent thrombosis (ST) is related to high rates of cardiac reinfarction. We present a case of reinfarction from ST.
Written by Jesse McLaren A 70 year old with prior MIs and stents to LAD and RCA presented to the emergency department with 2 weeks of increasing exertional chestpain radiating to the left arm, associated with nausea. Int J Cardiol 2024 3. Eur Heart J Digital Health 2024 5. Amsterdam et al. Circulation 2014 2.
P.S.: Cardiac cath was performed — and showed a distal LA D "culprit" lesion that was successfully stented. The following are the KEY clinical and ECG features that establish the diagnosis of W ellens ' S yndrome : There should be a history of prior chestpain that has resolved at the time the defining ECG is obtained.
Sent by anonymous A man in his 40s with no previous heart disease presented within 30 minutes of onset of acute chestpain that started while exercising. Successful drug-eluting stent placement opening up 95% mid RCA stenosis to 0% residual Nonobstructive left system disease. Chestpain and a computer ‘normal’ ECG.
ChestPain – Benign Early Repol or OMI? Written by Destiny Folk, MD, Adam Engberg, MD, and Vitaliy Belyshev MD A man in his early 60s with a past medical history of hypertension, type 2 diabetes, obesity, and hyperlipidemia presented to the emergency department for evaluation of chestpain.
The impact of this narrowing can ultimately result in angina (chestpain), which has been shown to double the risk of major cardiovascular events,1 as well as myocardial infarction ( heart attack ) or even death. Accessed May 2024. For more information: www.gehealthcare.com References: 1 World Health Federation.
On the second morning of his admission, he developed 10/10 chestpain and some diaphoresis after breakfast. The patient was given opiates which improved his chestpain to 7/10. The consulting cardiologist wrote in their note: “Could be cardiac chestpain. She is usually incredibly good at recognizing them!
A prehospital “STEMI” activation was called on a 75 year old male ( Patient 1 ) with a history of hyperlipidemia and LAD and Cx OMI with stent placement. He arrived to the ED by helicopter at 1507, about three hours after the start of his chestpain while chopping wood around noon. It was stented. This was a large OMI.
On the day of presentation she complained of typical chestpain, and stated it feels like prior MI. At that visit the patient was found to have an in-stent RCA occlusion. The patient was referred emergently to the cath lab, and again there was an in-stent RCA occlusion. What do you think? Troponin I peaked at 18.323ng/L.
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chestpain relieved by rest. This episode of chestpain began 3 hours ago and was persistent even at rest. Troponin was ordered.
Sent by anonymous, written by Pendell Meyers Case 1: A man in his 50s presented with acute chestpain. The cath lab was activated, and then not cancelled, and the angiogram showed 99% TIMI 2 flow proximal LAD culprit lesion, stented in less than 90 minutes of arrival. Normal vital signs. Normal vitals. What do you think?
This patient had the onset of chestpain 24 hours before arrival to the ED. The door to balloon time was incredibly short and there was a 100% circumflex occlusion that was opened and stented. For more on ECG findings in pulmonary disease — Check out My Comment in the May 31, 2024 post in Dr. Smith's ECG Blog ).
He reported typical chestpain since 4H AM and arrived at our ED at 10h with ongoing chestpain. Successful primary angioplasty of the mid-circumflex artery towards the main marginal branch with the implantation of a drug-eluting stent. You must record frequent serial ECGs for patients with chestpain.
Circulation, Volume 150, Issue Suppl_1 , Page A4145631-A4145631, November 12, 2024. This was treated with a drug-eluting stent, but TIMI 3 flow was not achieved. Due to ongoing shock despite initial mechanical support, the patient was escalated to an Impella CP device after a transthoracic echo confirmed no left ventricle thrombus.
Circulation, Volume 150, Issue Suppl_1 , Page A4139995-A4139995, November 12, 2024. Patients without data on C-reactive protein and high-density lipoprotein cholesterol and those who had a history of coronary artery bypass grafting and stenting in the left anterior descending artery were excluded. Recently, Rinaldi et al.
The patient said his chestpain was 4/10, down from 8/10 on presentation. On the combined basis of angiography and IVUS, this patient received stents to his mid RCA, proximal PDA, and OM. RCA and PDA before and after, arrows indicating stented regions. OM before and after, arrow indicating stented region.
No patient with chestpain should be sent home without troponin testing. All three lesions had TIMI 2 flow prior to stenting. This is an RAO cranial projection of the left coronary vessels after thrombectomy and stenting. The patient was sent home with a prescription for omeprazole to treat presumed peptic disease.
Written by Willy Frick A 40 year old woman was at home cooking when she developed chestpain. The operator documented thoughtful consideration of risks and benefits of stent placement. Technically, there was a very narrow landing zone for the stent, and missing this could result in "jailing" the LCx, which is ideally avoided.
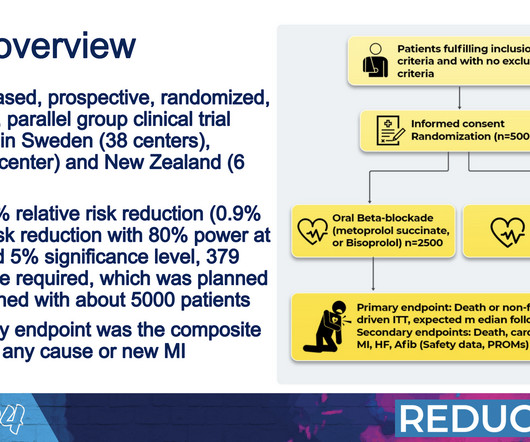
At that time, the damage to the heart muscle was greater than we see today, and we didn’t have the possibility to revascularize patients with percutaneous coronary intervention and stents like we do today,” Yndigegn said. Over a median follow-up period of 3.5
The patient is female in her 80s with a medical hx of previous MI with PCI and stent placement. She presented to the emergency department after a couple of days of chest discomfort. She also has a hx of paroxysmal atrial fibrillation and is on oral anticoagulant treatment. The last echocardiography 12 months ago showed HFmrEF.
Written by Willy Frick A 51 year old man with hypertension presented with three hours of acute onset, severe midsternal chestpain associated with two episodes of nausea and vomiting. or 2) Inferior and lateral OMI that is beginning to reperfuse, even though the patient still has chestpain? ECG 1 What do you think?
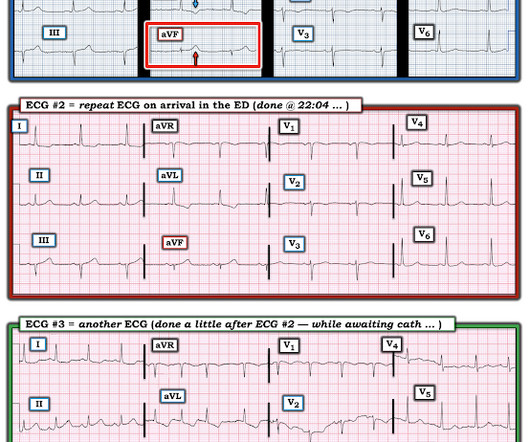
All of the patients contacted EMS due to acute onset chestpain. The above ECG is from a 70 something male with chestpain. ECG #2 Case 2 : The above ECG was obtained from a diabetic 45 year old smoker with chestpain. Following the improvement in the ECG the patient's pain too improved drastically.
Written by Pendell Meyers An elderly female called EMS with acute chestpain. Putting It All Together As per Dr. Meyers the case ended well with cardiac cath showing an RCA "culprit" which was successfully stented. Her vitals were within normal limits, and here is her EMS ECG: What do you think?
Written by Willy Frick A young woman with a history of paroxysmal nocturnal hemoglobinuria presented with acute substernal chestpain. The report describes heavy plaque in the proximal RCA by IVUS, but no lesions in the previously occluded RPL branch and no stent was deployed. Smith : The cath lab should be activated now!
Dizziness is so unlikely to be OMI without an obvious ECG, that I am going to pretend that this patient presented with chestpain. So let's pretend this is acute chestpain. In the November 27, 2024 post Drs. If no, then she will tell you that the case is outside of the intended use group. What do you think?
This was texted to me by a paramedic while I was out running one day: "54 yo male chestpain started at 1pm. History of diabetes type II and stent placement in 2018. I’m seeing hyperacute T waves III, aVF, down sloping depression I and aVL. What do you think? I responded: "Definite inferior OMI. And Right Ventricular.
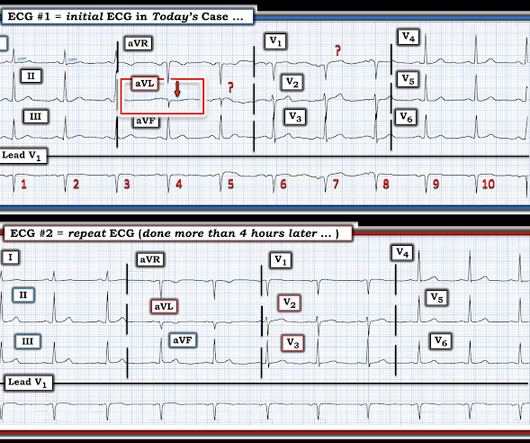
Written by Magnus Nossen The below ECG was obtained from a 65 year old man with ongoing chestpain. The below ECG was obtained 45 minutes after the first one with the patient being free of chestpain at the time of recording of ECG #2. He remained chestpain free and underwent coronary angiography the following day.
The patient contacted the ambulance service after he experienced sudden onset chestpain and diaphoresis that had started 20 minutes prior. At cath there was a 100% proximal LAD occlusion, which was opened and stented. The above ECG is from man in his 80s with crushing chestpain. 2024, January 31).
Written by Willy Frick A man in his 60s with hypertension and prior stroke presented with three days of crushing chestpain. He reported intermittent chestpain for the last few months, but never lasting this long. The cardiology consultant notes that pain is "almost resolved." There is active infarction.
Case A 68 year old man with a medical history of hypertension, hyperlipidemia, and CAD with stent deployment in the RCA presented to the emergency department with chestpain. After stent placement: The vessel is now open with TIMI 3 flow, although it is diffusely diseased and the middle segment is ectatic.
Written by Pendell Meyers, few edits by Smith A woman in her 70s was woken from sleep by midsternal chestpain radiating to left arm with nausea. My Comment , by K EN G RAUER, MD ( 11/10 /2024 ): = Think of today's case as a check of your skill in recognizing when to activate the cath lab. Queen of hearts explainability image.
1) Very high initial troponin of 45,000 ng/L 2) A full day of chestpain 3) Q-waves on the ECG, with some T-wave inversion Here is one frame of the CT scan which includes the heart: Can you spot the infarct? It was opened and stented. The November 8, 2024 post — artifact complicating OMI assessment. How do I know?
This was submitted by a paramedic, Hailey Kennedy A late 50s male called 911 following 2 hours of chestpain that started while working at his desk. He reported the crushing chestpain radiated down his left arm. He presented to the ED for evaluation chestpain. Pain was improved but not gone upon arrival.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.










































Let's personalize your content