This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
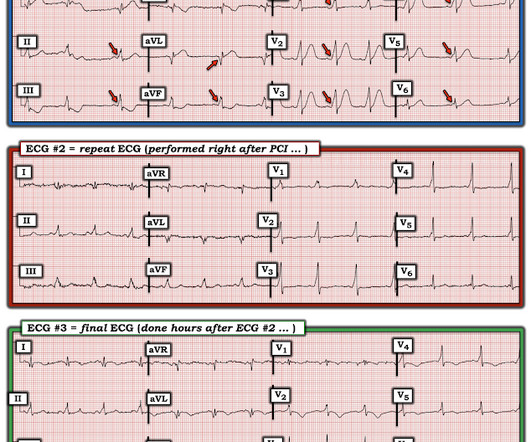
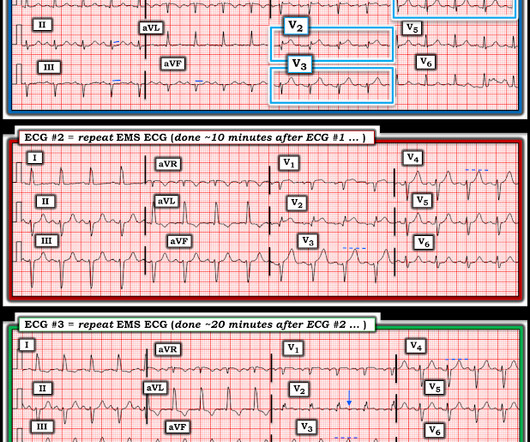
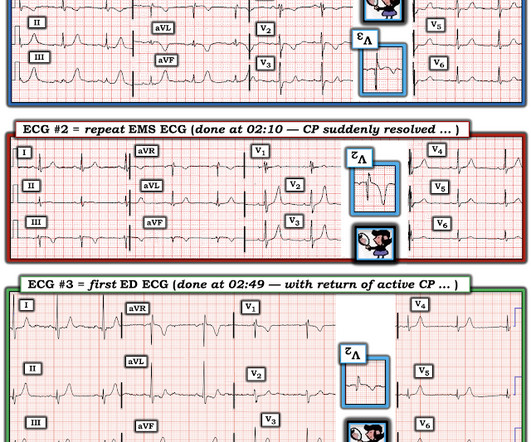
Written by Jesse McLaren A 45-year-old presented with 24 hours of intermittent chestpain. On it’s own this is nonspecific, but in the right context this could be diagonal occlusion (if active chestpain) or infero-posterior reperfusion (if resolved chestpain). #2 Can you guess the sequence?
Written by Jesse McLaren, with a very few edits by Smith A 60-year-old presented with chestpain. The ECG did not meet STEMI criteria, and the final cardiology interpretation was “ST and T wave abnormality, consider anterior ischemia”. But STEMI criteria is only 43% sensitive for OMI.[1]
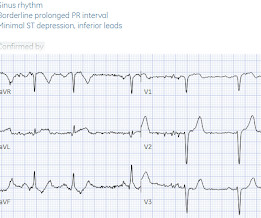
Written by Jesse McLaren A healthy 75 year old developed 7/10 chestpain associated with diaphoresis and nausea, which began on exertion but persisted. Below is the first ECG recorded by paramedics after 2 hours of chestpain, interpreted by the machine as “possible inferior ischemia”. What do you think?
Written by Pendell Meyers A man in his 60s presented with acute chestpain and normal vital signs. Its hard to measure the STE in I exactly with the moving baseline, but there is almost certainly not enough STE to meet STEMI criteria. Here is his triage ECG: What do you think? They are symmetric, fat, convex on both sides, etc.
Written by Jesse McLaren A previously healthy 60 year old developed exertional chestpain with diaphoresis, and called EMS. So while there’s no diagnostic STEMI criteria, there are multiple ischemic abnormalities in 11/12 leads involving QRS, ST and T waves, which are diagnostic of a proximal LAD occlusion. What do you think?
Written by Jesse McLaren, comments by Smith A 55 year old with a history of NSTEMI presented with two hours of exertional chestpain, with normal vitals. See these posts: ChestPain, ST Elevation, and an Elevated Troponin: Should we Activate the Cath Lab? So this NSTEMI was likely a STEMI(-)OMI with delayed reperfusion.
Written by Willy Frick A man in his 50s with history of hypertension, hyperlipidemia, and a 30 pack-year smoking history presented to the ER with 1 hour of acute onset, severe chestpain and diaphoresis. For national registry purposes, this will be incorrectly classified as a STEMI.) Most STEMI have peak cTnI greater than 10.0.
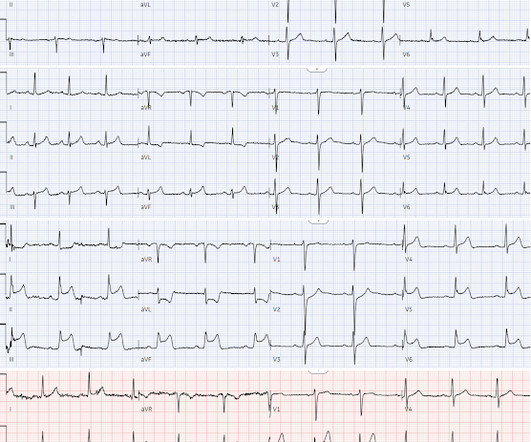
Written by Magnus Nossen with Edits by Grauer and Smith The ECGs in today’s case are from 3 different patients all presenting with new-onset CP ( ChestPain ). It definitely does not fulfill STEMI criteria, and I would argue that it would not lead to cath lab activation in most centers. The ECG shows ST depression in lead V3.
Written by Jesse McLaren A 50 year old presented to triage with one hour of chestpain, and the following ECG labeled normal by the computer (GE Marquette SL) algorithm. Smith comment: we showed that the first troponin, even in full-blown STEMI, is negative 25% of the time. What do you think?
I was working at triage when the medics brought this patient who is 65 yo and has had chestpain for 12 hours. The pain had been intermittent until an hour before arrival, when he called 911. Another ECG was recorded while awaiting the cath team: Now there is STEMI Let's look at that first (prehospital ECG) again: Very subtle!
A 50-something male with hypertension and 20- to 40-year smoking history presented with 1 week of stuttering chestpain that is worse with exertion, which takes many minutes to resolve after resting and never occurs at rest. At times the pain does go to his left neck. What do you think the prehospital ECG showed (with pain)?
Written by Jesse McLaren Two patients in their 70s presented to the ED with chestpain and RBBB. Patient 1 : a 75 year old called paramedics with one day of left shoulder pain which migrated to the central chest, which was worse with deep breaths. Do either, both, or neither have occlusion MI? Vitals were normal.
Written by Pendell Meyers A woman in her 70s had acute chestpain and called EMS. Interpretation : diagnostic of acute anterior OMI with STE less than STEMI criteria in V1-V4, hyperacute T waves in V2-V4, and suspiciously flat isoelectric ST segments in III and aVF suspicious for reciprocal findings. Ongoing OMI.
Case An 82 year old man with a history of hypertension presented to the ED with chestpain at 1211. He described his chestpain as pleuritic and reported that it started the day prior while swinging a golf club. His pain suddenly became much worse in the ED and he became acutely diaphoretic, dizzy, and hypotensive.
A healthy 45-year-old female presented with chestpain, with normal vitals. The patient was previously healthy, with no atherosclerotic risk factors, and developed chestpain after an episode of stress. The pain was crushing retrosternal, radiated to the arms and was associated with lightheadedness.
Written by Jesse McLaren A 70 year old with prior MIs and stents to LAD and RCA presented to the emergency department with 2 weeks of increasing exertional chestpain radiating to the left arm, associated with nausea. I sent this to the Queen of Hearts So the ECG is both STEMI negative and has no subtle diagnostic signs of occlusion.
Sent by anonymous A man in his 40s with no previous heart disease presented within 30 minutes of onset of acute chestpain that started while exercising. Now it is a full blown STEMI of 3 myocardial territories: inferior, posterior, and lateral But at least it does not call it "Normal." Chestpain and a computer ‘normal’ ECG.
It has been estimated that in the aggregate, they occur at a rate of about 3 per 1000 patients with acute MI, and most of these events occur in patients with STEMI. A mong patients with STEMI, ventricular septal rupture is the most common and free wall rupture is the least common.
A prehospital “STEMI” activation was called on a 75 year old male ( Patient 1 ) with a history of hyperlipidemia and LAD and Cx OMI with stent placement. He arrived to the ED by helicopter at 1507, about three hours after the start of his chestpain while chopping wood around noon. He wrote most of it and I (Smith) edited.
Prompt cath is therefore advised if the post-ROSC shows an acute STEMI. To Emphasize: The phenomenon of T-QRS-D is not needed in today's case to recognize the acute STEMI. Once the J-point is recognized in the chest leads ( RED arrows in leads V2,V3,V4 of Figure-2 ) — the marked ST elevation becomes obvious.
He reports significant chestpain at the base of his scapula on the right side along with new shortness of breath. Smith : there is some minimal ST elevation in V2-V6, but does not meet STEMI criteria. Transient STEMI has been studied and many of these patients will re-occlude in the middle of the night. Is it normal STE?
Written by Willy Frick A 50 year old man with no medical history presented with acute onset substernal chestpain. This was a machine read STEMI positive OMI. We've highlighted a considerable number of acute RV MI cases in Dr. Smith's ECG Blog ( See the October 7, 2019 and May 10, 2024 posts , to name just two ).
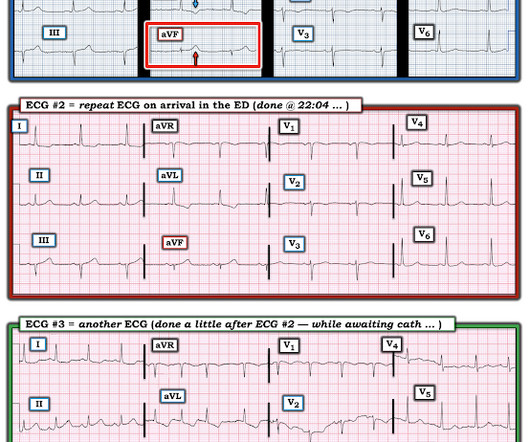
Written by Pendell Meyers A man in his early sixties with no significant medical history (including a "negative cardiac workup a few years ago" for unclear indication) called 911 for acute chestpain constantly for the past 5 hours. However, this patient has active chestpain, and thus this this is inferior-posterior OMI.
Even without ECG changes — persistent ischemic-sounding chestpain is indication for prompt cath. ECG Blog #193 — Reviews the basics for predicting the " culprit " artery ( as well as reviewing why the term "STEMI" — should be replaced by "OMI" = O cclusion-based MI ).
Just as important is pretest probability: did the patient report chestpain prior to collapse? Cardiac arrest #3: ST depression, Is it STEMI? or is he an ACCESS Trial Candidate? == MY Comment , by K EN G RAUER, MD ( 7/5 /2024 ): == Clinical ECG interpretation is a 2-Step process. Then assume there is ACS.
Written by Bobby Nicholson What do you think of this “STEMI”? Second, although there is a lot of ST Elevation which meets STEMI criteria, especially in V3-4, the ST segment is extremely upwardly concave with very large J-waves (J-point notching). With EMS, patient had a GCS of 3 and was saturating 60% on room air. ng/mL and 0.10
My New E CG P odcasts ( 5/28/2024 ): These podcasts are part of the Mayo Clinic Cardiovascular CME Podcasts Series ( "Making Waves" ) — hosted by Dr. Anthony Kashou. 2:00 — Dr. Kashou to Dr. Grauer: "In 2024 — Where do you see computerized ECG interpretations and AI?" 2:50 — Let’s start with comparison of 12-Lead ECGs.
On the second morning of his admission, he developed 10/10 chestpain and some diaphoresis after breakfast. The patient was given opiates which improved his chestpain to 7/10. The consulting cardiologist wrote in their note: “Could be cardiac chestpain. She is usually incredibly good at recognizing them!
Here is his ED ECG at triage: Obvious high lateral OMI that does not quite meet STEMI criteria. He was given aspirin and sublingual nitro and the pain resolved. The history is concerning ( This patient was awakened from sleep by chestpain that persisted for several hours — on a background of intermittent CP in recent weeks ).
QOH versions 1 and 2 both say Not OMI, with high confidence, without any clinical context, despite the abnormal STE meeting STEMI criteria. Context: a man in his 40s presented to the emergency department with 1 day of sudden onset chestpain. I sent this to our group without information and Dr. Smith responded: "Not OMI.
The conventional machine algorithm interpreted this ECG as STEMI. See this post of RV MI with both McConnell sign and "D" sign: Inferior and Posterior STEMI. But the History in today's case was acute shortness of breath with dizziness and lightheadedness — and, essentially without chestpain!
This patient had the onset of chestpain 24 hours before arrival to the ED. The Non-STEMI, which was an OMI, was diagnosed much faster with AI on the ECG than with troponin. For more on ECG findings in pulmonary disease — Check out My Comment in the May 31, 2024 post in Dr. Smith's ECG Blog ).
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chestpain relieved by rest. This episode of chestpain began 3 hours ago and was persistent even at rest. Troponin was ordered.
Later, I found old ECGs: 5 month prior in clinic: V5 and V6 look like OMI 9 months prior in clinic with no chest symptoms: V5 and V6 look like OMI 1 year prior in the ED with chestpain: V5 and V6 sure look like a STEMI For this ECG and chestpain in the ED, the Cath lab activated. There was no OMI.
A 55 year old with no previous cardiac history presented with 3 hours of chestpain. The pain was persistent and reportedly still present at the time of the ECG. But if the pain is persistent, as reported, then the patient must go to the cath lab even if the ECG suggests reperfusion.
Sent by anonymous, written by Pendell Meyers Case 1: A man in his 50s presented with acute chestpain. Click here to sign up for Queen of Hearts Access Case 2: A woman in her 60s presented with acute chestpain. Another missed OMI by the False STEMI-NonSTEMI Dichotomy Don't miss them!!! Normal vital signs.
The patient said his chestpain was 4/10, down from 8/10 on presentation. Sometimes it can take 12 or 24 hours to see ECG evidence of reperfusion. == MY Comment , by K EN G RAUER, MD ( 1/4/ 2024 ): == Superb and thorough discussion by Dr. Frick of today's case! Remember that patients with OMI can have normal ECGs!
Easy LINK — [link] — My New E CG P odcasts ( 5/28/2024 ): These podcasts are part of the Mayo Clinic Cardiovascular CME Podcasts Series ( "Making Waves" ) — hosted by Dr. Anthony Kashou. 2:25 — Dr. Grauer: The 1st Error : Too many clinicians in 2024 are still stuck in the outdated millimeter-based STEMI Paradigm”.
Written by Pendell Meyers A man in his 40s called EMS for acute chestpain that awoke him from sleep, along with nausea and shortness of breath. Learning Points: Currently by definition, there is unfortunately no such thing as a formal diagnosis of STEMI or STEMI criteria in the setting of RBBB and LAFB.
Written by Colin Jenkins and Nhu-Nguyen Le with edits by Willy Frick and by Smith A 46-year-old male presented to the emergency department with 2 days of heavy substernal chestpain and nausea. The patient continued having chestpain. Is there STEMI? Fortunately the patient was then taken for angiography.
Written by Jesse McLaren Two patients presented with acute chestpain, and below are the precordial leads V1-6 for each. Patient 1 Patient 2 STEMI criteria is based only ST elevation millimeter criteria measured in isolation from the QRS and stratified by age/sex, so this is the only information provided above.
Written by Pendell Meyers, with edits by Smith A man in his 80s presented with acute chestpain and normal vital signs. It was read by the treating physician and the overreading cardiologist as "Paced, no STEMI." Here is his triage ECG at time = 0: What do you think? (No How does the Queen of Hearts do? 2021;23:187.
Written by Pendell Meyers A man in his late 30s with history of hypertension, tobacco use, and obesity presented to the Emergency Department for acute chestpain which started approximately 3 hours prior to arrival, in the setting of a very stressful situation. The pain radiated down both arms, 10/10 in severity.
ChestPain – Benign Early Repol or OMI? Written by Destiny Folk, MD, Adam Engberg, MD, and Vitaliy Belyshev MD A man in his early 60s with a past medical history of hypertension, type 2 diabetes, obesity, and hyperlipidemia presented to the emergency department for evaluation of chestpain.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.












































Let's personalize your content