This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Written by Jesse McLaren, with a very few edits by Smith A 60-year-old presented with chestpain. Inferior hyperacute T waves, which have been added to the 2022 ACC consensus on chestpain as a “STEMI equivalent”[3] 3. Int J Cardiol 2024 2. But are there any other signs of Occlusion MI? Nikus et al. Kontos et al.
I assumed it was a patient with acute chestpain. It was a man in his 30s with chestpain. Performance of Artificial Intelligence Powered ECG Analysis in Suspected ST-Segment Elevation MyocardialInfarction. This was sent to me from Sam Ghali ( @EM_Resus ) with no other information. What do you think, Steve?
Written by Colin Jenkins and Nhu-Nguyen Le with edits by Willy Frick and by Smith A 46-year-old male presented to the emergency department with 2 days of heavy substernal chestpain and nausea. The patient continued having chestpain. These diagnoses were not found in his medical records nor even a baseline ECG.
A 50-something male with hypertension and 20- to 40-year smoking history presented with 1 week of stuttering chestpain that is worse with exertion, which takes many minutes to resolve after resting and never occurs at rest. At times the pain does go to his left neck. It is a ssociated with mild dyspnea on exertion. Am Heart J.
Written by Magnus Nossen with Edits by Grauer and Smith The ECGs in today’s case are from 3 different patients all presenting with new-onset CP ( ChestPain ). The ECG is diagnostic of occlusion myocardialinfarction (OMI). All ECGs were recorded by EMS, and transferred to a PCI capable center for evaluation.
No ChestPain, but somnolent. The fact that this is syncope makes give it a far lower pretest probability than chestpain, but it was really more than syncope, as the patient actually underwent CPR and had hypotension on arrival of EMS. 2) — How to distinguish between LV aneurysm vs new infarction ?
A 60-something male presented stating that he had had chestpain that morning which awoke him from sleep but then resolved after several minutes. He has had similar pain in the past which he attributed to acid reflux. He is pain free now. The patient is pain free at the time of this ECG: What do you think?
5 Revascularization to improve blood flow to the heart has been shown to reduce mortality in stable chestpain patients. 5 Revascularization to improve blood flow to the heart has been shown to reduce mortality in stable chestpain patients. 2024, [link]. Journal of Vascular Surgery, Mar.
This is a value typical for a large subacute MI, n ormal value 48 hours after myocardialinfarction is associated with Post-Infarction Regional Pericarditis ( PIRP ). Mechanical complications secondary to myocardialinfarction are infrequent due to most patients receiving revascularization quite rapidly.
This confirms that the pain was ischemia and is now resovled. Thus, it has recently become generally accepted that most plaque ruptures resulting in myocardialinfarction occur in plaques that narrow the lumen diameter by 40% of the arterial cross section may be involved by plaque. The i nitial hs troponin I returned 75%.
He reports significant chestpain at the base of his scapula on the right side along with new shortness of breath. Timing of revascularization in patients with transient ST segment elevation myocardialinfarction: a randomized clinical trial. See these casese (and I have many others): First ED ECG is Wellens' (pain free).
Written by Jesse McLaren A 70 year old with prior MIs and stents to LAD and RCA presented to the emergency department with 2 weeks of increasing exertional chestpain radiating to the left arm, associated with nausea. Int J Cardiol 2024 3. Eur Heart J Digital Health 2024 5. Lupu et al. Clin Cardiol 2022 4.
Circulation, Volume 150, Issue Suppl_1 , Page A4134796-A4134796, November 12, 2024. Introduction:Over 6 million patients (pts) present to US emergency departments annually with chestpain (CP), of which the majority are found to have no serious disease. Length of stay (LOS) in the CPU to discharge was 10.4
The impact of this narrowing can ultimately result in angina (chestpain), which has been shown to double the risk of major cardiovascular events,1 as well as myocardialinfarction ( heart attack ) or even death. Accessed May 2024. For more information: www.gehealthcare.com References: 1 World Health Federation.
Image courtesy: ACC christine.book Thu, 02/29/2024 - 11:22 February 29, 2024 — The American College of Cardiology ( ACC ) will soon be holding its ACC 73rd Annual Scientific Session & Expo , ACC.24 24 from April 6 - 8, 2024 in Atlanta, GA at the Georgia World Congress Center.
Getty Images milla1cf Thu, 01/25/2024 - 20:44 January 25, 2024 — Agepha Pharma , a leading multinational pharmaceutical company with the first FDA-approved anti-inflammatory cardiovascular treatment ( LODOCO – colchicine, 0.5 More than 8 million Americans visit hospital emergency departments experiencing chestpain every year.
tim.hodson Tue, 10/15/2024 - 12:12 Oct. 15, 2024 – Elucid has announced that four of the seven Medicare Administrative Contractors (MACs) will extend coverage for AI-enabled quantitative coronary plaque analysis, including its FDA-cleared PlaqueIQ image analysis software, beginning Nov.
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chestpain relieved by rest. This episode of chestpain began 3 hours ago and was persistent even at rest. Troponin was ordered. Eur J Emerg Med.
By Magnus Nossen, edits by Grauer and Smith The patient is a 70-something female with DMII, HTN and an extensive prior history of coronary artery disease and myocardialinfarctions. On the day of presentation she complained of typical chestpain, and stated it feels like prior MI. She's had multiple PCI procedures.
Circulation, Volume 150, Issue Suppl_1 , Page A4135360-A4135360, November 12, 2024. Case presentation:A 64-year-old man presented with one day of chestpain. TTE showed a reduced EF with multiple segmental abnormalities concerning for myocardialinfarction. Electrocardiogram (EKG) was unremarkable.
Additionally, 2D transthoracic echocardiography (TTE), and myocardial injury serum biomarkers assays (creatine phosphokinase-MB [CPK-MB] and cardiac troponins [cTn]) were measured once. The most common symptom was left hemithorax and interscapular pain (317 patients, 46%).
He reported typical chestpain since 4H AM and arrived at our ED at 10h with ongoing chestpain. You must record frequent serial ECGs for patients with chestpain. Immediate and early percutaneous coronary intervention in very high-risk and high-risk non-ST segment elevation myocardialinfarction patients.
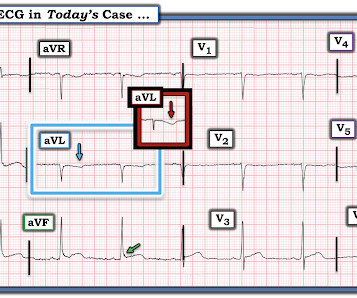
Sometimes arrhythmogenic cardiomyopathy patients can present with acute chestpain and elevation of myocardial enzymes and has been called as ‘hot phase’ These require differentiation from acute myocardialinfarction and have normal coronary arteries [3]. 2024 Feb 27;83(8):797-807. 2023.12.015.
Terminal QRS distortion is present in anterior myocardialinfarction but absent in early repolarization. PMID: 27658331. == MY Comment , by K EN G RAUER, MD ( 10/6 /2024 ): == I found today’s 2 ECGs remarkable for a number interesting findings — including the reasons why I thought acute OMI unlikely. Lee DH, Walsh B, Smith SW.
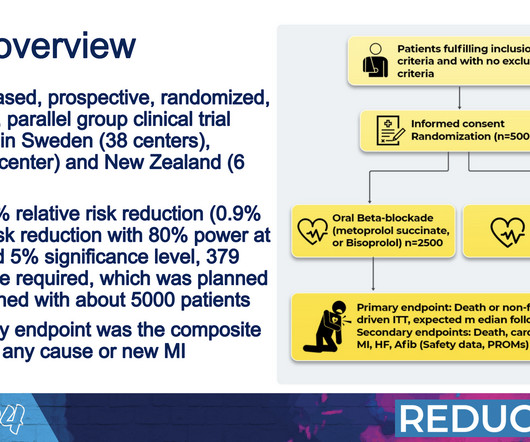
What we see today is more myocardialinfarctions that are smaller and that do not damage the heart muscle to the same extent.” Over a median follow-up period of 3.5 There were also no differences in safety endpoints such as stroke, abnormally low blood pressure or fainting.
Circulation, Volume 150, Issue Suppl_1 , Page A4119169-A4119169, November 12, 2024. She was diagnosed with NSTEMI with a thrombolysis in myocardialinfarction (TIMI) score of 5. PCI has become a common treatment of chronic total occlusion, and techniques continue to be developed to tackle more challenging cases.
A 55 year old with no previous cardiac history presented with 3 hours of chestpain. The pain was persistent and reportedly still present at the time of the ECG. Translation from French: Acute Occlusion MyocardialInfarction with High Confidence. He has now implemented the Queen of Hearts in his hospital.
Circulation, Volume 150, Issue Suppl_1 , Page A4140337-A4140337, November 12, 2024. The confirmation cohort, which was obtained from the National Institute of Health, consisted of 3315 patients with normal Bruce protocol treadmill stress test results in the Prospective Multicenter Imaging Study for Evaluation of ChestPain (PROMISE) Trial.
Case A 43 year old male with a history of DM II, hyperlipidemia, and a family history of myocardialinfarction presented to a family clinic with two days of epigastric pain that started after consuming a meal. He described the pain as a “crushing and discomforting” feeling with no radiation.
So there is probability of myocardial injury here (and because it is in the correct clinical setting, then myocardialinfarction.) The patient said his chestpain was 4/10, down from 8/10 on presentation. HsTnI drawn at that time was 9 ng/L (ref. 80%) and definitely too much for hour to hour.
The patient in today’s case is a previously healthy 40-something male who contacted EMS due to acute onset crushing chestpain. The pain was 10/10 in intensity radiating bilaterally to the shoulders and also to the left arm and neck. Written By Magnus Nossen — with edits by Ken Grauer and Smith. The below ECG was recorded.
Written by Pendell Meyers, with edits by Smith A man in his 80s presented with acute chestpain and normal vital signs. We need more such ECGs for training but we are constantly working on the algorithm and one day it will make this diagnosis. == But isn't ongoing chestpain in NSTEMI a guideline indication for emergent angiography?
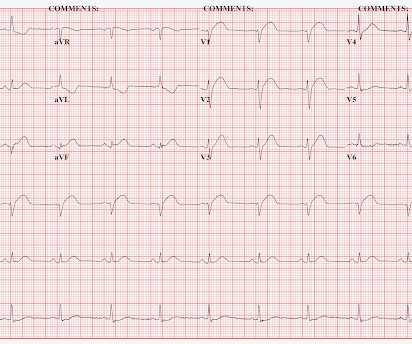
Written by Jesse McLaren Two patients presented with acute chestpain, and below are the precordial leads V1-6 for each. Hyperacute T waves can be a useful sign of occlusion myocardialinfarction if appropriately defined. Acad Emerg Med 2023 3. Smith, Meyers. Ann Emerg Med 2023 4. Meyers, Bracey et al.
All of the patients contacted EMS due to acute onset chestpain. The above ECG is from a 70 something male with chestpain. ECG #2 Case 2 : The above ECG was obtained from a diabetic 45 year old smoker with chestpain. He arrived in our ED with the below ECG pain free. Which of the ECGs represent OMI?
Scenario 1 : The patient presents with 24 hours of substernal chestpain. It could also, given a different clinical context be compatible with a subacute myocardialinfarction complicated by post infarct regional pericarditis. Most common cause) 2 ) Post infarct regional pericarditis. What do you think?
Case 1: 20-something woman with chestpain Case 2: 50-something man with chestpain Case 1 A 20-something yo woman presented in the middle of the night with severe crushing chestpain. History Patient complains of a 24-hours of chestpain of sudden onset, sharp in nature. Denies SOB.
Written by Magnus Nossen The below ECG was obtained from a 65 year old man with ongoing chestpain. The below ECG was obtained 45 minutes after the first one with the patient being free of chestpain at the time of recording of ECG #2. He remained chestpain free and underwent coronary angiography the following day.
The patient contacted the ambulance service after he experienced sudden onset chestpain and diaphoresis that had started 20 minutes prior. of patients with anterior myocardialinfarction ( 1 ). Tall precordial T waves with depressed ST take-off: an early sign of acute myocardialinfarction?
This was texted to me by a paramedic while I was out running one day: "54 yo male chestpain started at 1pm. Let's see how the PMCardio Queen of Hearts AI Model performs: "Acute Occlusive MyocardialInfarction" She gave this a score of 1.0 (100% History of diabetes type II and stent placement in 2018. What do you think?
A 50-something man presented with worsening severe exertional chestpain which was just resolving as he had an ECG recorded in triage. Are the T-waves in leads I and II hyperacute? Hard to tell. How can we know? By the evolution of the ECG! Watch what happends as the heart recovers from its episode of ischemia.
He denied chestpain. It is correct that he did not have chestpain, but we must remember that fully 1/3 of full blown STEMI do not present with chestpain. They made a final diagnosis of type II myocardialinfarction. Bedside POCUS showed very poor LV function and a few pulmonary B lines.
tim.hodson Wed, 10/30/2024 - 11:23 Oct. 27, 2024 — HeartFlow, Inc. The data show the HeartFlow platform provides clinicians with the insights needed to anticipate and mitigate adverse events, including myocardialinfarctions, in symptomatic patients with stable chestpain.
1) Very high initial troponin of 45,000 ng/L 2) A full day of chestpain 3) Q-waves on the ECG, with some T-wave inversion Here is one frame of the CT scan which includes the heart: Can you spot the infarct? The November 8, 2024 post — artifact complicating OMI assessment. This is then a large MI, but it is subacute.
Methods This cross-sectional study included 585 consecutive Chinese patients (age ≥18 year) who presented to an emergency department with chestpain (lasting >5 min) and were managed following the chestpain protocol between 1 August 2023 and 12 June 2024.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.














































Let's personalize your content