This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
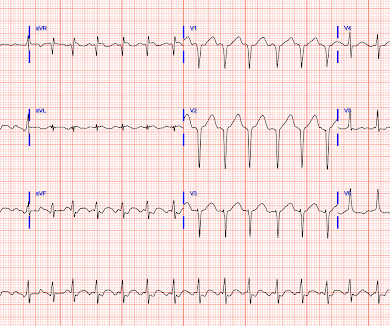
A 55-year-old man had an out-of-hospital cardiacarrest. An evaluation showed 2-mm ST-segment elevations in the inferior leads on electrocardiography, cardiogenicshock, and a new systolic murmur. A diagnosis was made.
Figure B At this point, with the ECG changing from diffuse ST depression to widespread ST elevation and the patient presenting in cardiogenicshock, left main coronary artery (LMCA) occlusion is the likely diagnosis. This patient is actively dying from a left main coronary artery OMI and cardiacarrest from VT/VF or PEA is imminent!
Written by Pendell Meyers A man in his 50s was found by his family in cardiacarrest of unknown duration. His family started CPR and called EMS, who arrived to find him in ventricular fibrillation. 15 minutes after EMS arrival, after at least 6 defibrillations, the patient achieved sustained ROSC.
Some patients have baseline RBBB with LAFB, but in patients with likely ACS, these are associated with severe infarction with cardiacarrest, cardiogenicshock or impending shock. Suffice it to say that, "The heart does whatever it will do when a patient is about to arrest".
milla1cf Mon, 04/08/2024 - 18:07 April 8, 2024 — Implantation of the Impella CP micro-axial flow pump in the hours after a heart attack significantly increased the rate of survival at six months among people suffering cardiogenicshock, according to a study presented at the American College of Cardiology ’s Annual Scientific Session.
About 45 minutes after the second EKG, the patient was found in cardiacarrest. A temporary pacemaker was implanted, and she was admitted to the ICU with cardiogenicshock. Later the next day, she went into cardiacarrest again. By the time I saw the repeat EKG, the patient was already in cardiacarrest.
Circulation, Volume 150, Issue Suppl_1 , Page A4118341-A4118341, November 12, 2024. Background:Opioid use has increased significantly in the past few decades, impacting cardiac and non-cardiac patients. There was a non-significant increased risk of cardiogenicshock (aOR 1.14, 95% CI 0.87 - 1.5,
The patient in today’s case presented in cardiogenicshock from proximal LAD occlusion, in conjunction with a subtotally stenosed LMCA. LAD — 100% proximal occlusion; with 70-89% mid-vessel narrowing. LCx — 50-69% stenosis of the 1st marginal branch; with 100% distal LCx occlusion. RCA — 100% proximal occlussion.
There was 100% proximal LAD occlusion with TIMI 0 flow, and cardiacarrest in the cath lab. Among others — See My Comment at the bottom of the page in the September 13, 2024 post of Dr. Smith's ECG Blog ). In today's case — Dr. McLaren adds a few "twists" to this clinical challenge. There is sinus tachycardia at ~100/minute.
Circulation, Volume 150, Issue Suppl_1 , Page A4145617-A4145617, November 12, 2024. Background:Cardiogenic shock (CS) has high morbidity and mortality rates. Regardless of CS type, Black patients were more likely to have cardiacarrest during hospitalization. 0.93), pLVAD (aOR: 0.79, 95%CI: 0.72-0.86),
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.















Let's personalize your content