This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
== Review of ECG Rhythms — MIS-C Case Report ( 9/5 /2024 ): == What follows below are my first impressions of the ECG rhythms sent to me from the Case Report by Dimah Jarmakani et al — of a 12-year old boy with MIS-C ( M ultisystem I nflammatory S yndrome in C hildren ). Hope this helps — :) ECG-3 — I see sinus bradycardia and arrhythmia.
Discontinue all negative chronotropic agents, since the risk of torsade is much higher with bradycardia or pauses. Smith Pacing in today's case is an effective intervention as doing so prevents the bradycardia and pauses that are likely to precipitate additional episodes of Torsades de Pointes. ( The plan: 1. J Am Coll Cardiol.
Altered Mental Status, Bradycardia == MY Comment , by K EN G RAUER, MD ( 2/2 /2024 ): == Dr. Meyers began today’s case with the clinical challenge of asking you to identify the underlying cause of ECG #2. -- Read this ECG -- Osborn Waves and Hypothermia (this is the "Figure" above) What does LBBB look like in severe hypothermia?
EMS reports intermittent sinus tachycardia and bradycardia secondary to some type of heart block during transport. Limiting one's interpretation to marked bradycardia with high-grade AV block in need of pacing in this patient with multiple syncopal epiosodes — more than suffices for "the quick answer". Figure-3: I've labeled ECG #3.
I will leave more detailed rhythm discussion to the illustrious Dr. Ken Grauer below, but this use of calipers shows that the rhythm interpretation is: Sinus bradycardia with a competing (most likely junctional) rhythm. That is, until the 7th R wave which comes a little bit sooner than expected. Given the R-R interval = 1160 msecs.
Click here to sign up for Queen of Hearts Access == MY Comment , by K EN G RAUER, MD ( 9/11 /2024 ): == Among the important concepts brought out by today's case are the following: #1) — Is acute OMI a common cause of syncope ? #2) Former resident: "The biggest piece for me was the size of the T waves in relation to everything else.
Retrieved July 2, 2022, from [link] == MY Comment , by K EN G RAUER, MD ( 2/4 /2024 ): == Today's case by Dr. Meyers provides insight with regard to sequential evolution of serial ECGs during the course of cardiac contusion. Other Arrhythmias ( PACs, PVCs, AFib, Bradycardia and AV conduction disorders — potentially lethal VT/VFib ).
Looking first at the long-lead II rhythm strip — there is significant bradycardia , with a heart R ate just under 40/minute. But the point to emphasize — is that it should only take seconds to recognize that there is bradycardia from significant AV block. = Would you approve her for a nonemergent surgical procedure?
Whatever the specific etiology of today's arrhythmia is, the “good news” is — that this rhythm will most probably improve with reperfusion of the "culprit" artery. That said — I found today's arrhythmia fascinating, and worthy of more in-depth analysis. Using calipers facilitates the process.
Most of the time with AV block — the atrial rhythm will be regular ( or at least almost regular — if there is an underlying sinus arrhythmia ). PEARL # 5: As noted above — today's arrhythmia appears to represent some form of 2nd-degree AV block. Figure-4: I needed to draw a laddergram.
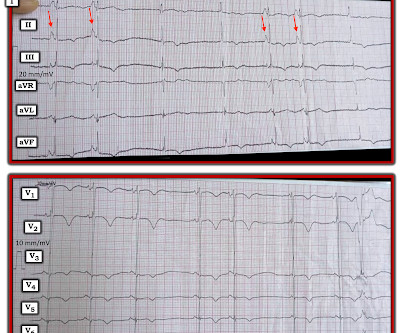
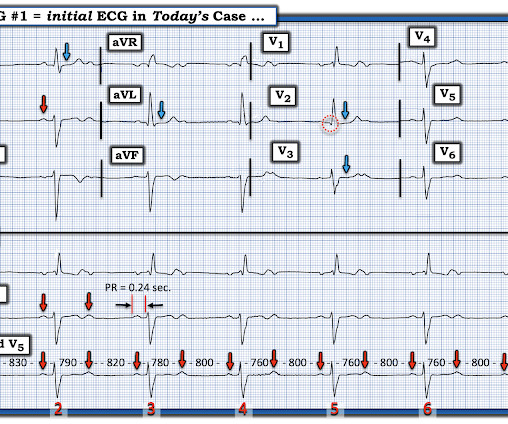
The Queen of Hearts AI app will hopefully be FDA approved in Q1 of 2024. I added, "Makes me wonder if this could be myocarditis in a younger adult — maybe even with sinus arrhythmia." It is already approved in Europe. YOU HAVE THE OPPORTUNITY TO GET EARLY ACCESS TO THE PM Cardio AI BOT!! Figure-1: The initial ECG in today's case.
Learning points : Takotsubo can lead to cardiac arrest from ventricular arrhythmia. Nossen highlights an important concept — namely pause -dependent precipitation of a malignant ventricular arrhythmia ( in this case Torsades de Pointes ).
Additionally, his cardiac telemetry monitor showed runs of accelerated idioventricular rhythm, a benign arrhythmia often associated with coronary reperfusion. He had multiple episodes of bradycardia and nonsustained ventricular tachycardia. As expected, the patient reported total resolution of pain by the time he got to the ED.
The ECG shows sinus bradycardia but is otherwise normal. Sometimes it can take 12 or 24 hours to see ECG evidence of reperfusion. == MY Comment , by K EN G RAUER, MD ( 1/4/ 2024 ): == Superb and thorough discussion by Dr. Frick of today's case! The documentation does not describe any additional details of the history.
Cardiology was consulted, and the note said "no arrhythmias on telemetry or pacer interrogation." This is supported by the PT note which described a palpably irregular pulse with pauses and marked bradycardia. The final cardiology recommendation was to increase fludrocortisone and midodrine.
However, he suddenly developed a series of malignant ventricular arrhythmias. Below are printouts of some of the arrhythmias recorded. This time, the arrhythmia did not spontaneously terminate — but rather degenerated to VFib, requiring defibrillation. The arrhythmia starts with a PVC having a short coupling interval.
There are three mechanisms of arrhythmia: automatic, re-entry, and triggered. The most common triggered arrhythmia is Torsades de Pointes. It is a benign arrhythmia which requires no specific treatment. Possible mechanisms of ventricular arrhythmias elicited by ischemia followed by reperfusion. Do not treat AIVR.
VT is the second most common presenting arrhythmia. Vaso or inotropic medications are not harmless, and can precipitate life threatening arrhythmias. It is common with 2nd- and 3rd-degree AV block to see a " ventriculophasic " sinus arrhythmia. AV block is the first manifestation of CS in more than 30% of patients.
The arrhythmia spontaneously converted before defibrillation was achieved. As per Dr. Nossen — today's initial ECG ( LEFT tracing in Figure-2 ) shows sinus bradycardia with QRS widening due to bifascicular block ( RBBB/LAHB ). The patient was rushed to the nearest emergency department (non-PCI facility) for stabilization.
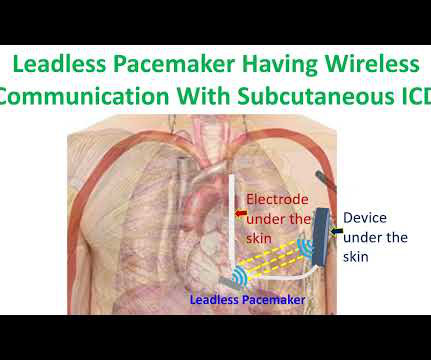
But subcutaneous ICD cannot provide bradycardia and antitachycardia pacing as a transvenous ICD. It was a multinational study which enrolled patients at risk for sudden death from ventricular arrhythmias and the follow up period was 6 months. None of the deaths in the study were deemed to be arrhythmia related or procedure related.
Vitals were within normal limits except bradycardia. Sinus bradycardia, normal QRS. These include the following: A fairly marked sinus arrhythmia with bradycardia, and almost the pattern of "group" beating in the long lead rhythm strip. See My Comment in the June 25, 2024 post for changes with LA-LL reversal ).
Learning points: Mobitz I and Mobitz II can co-exist in the same patient at the same time Bedside maneuvers can help clarify the etiology of 2:1 AV block == MY Comment , by K EN G RAUER, MD ( 11/10 /2024 ): == Questions often arise regarding the various forms of 2nd-degree AV block. Did YOU See the 2:1 AV Block?
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.























Let's personalize your content