This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
The logic of stenting obstructed coronary arteries is simple. A stent unblocks the artery. Subscribe now Stenting stable coronary artery disease has not been convincingly proven to reduce the risk of future heart attacks or death 1. But coronary stenting is not the only way to reduce symptoms of angina. All is fixed.
The Freesolve BTK RMS is designed for individuals suffering from chronic limb-threatening ischemia (CLTI). Updated estimates for the burden of chronic limb-threatening ischemia in the Medicare population, Journal of Vascular Surgery, Volume 77, Issue 6, 2023, 1760-1775 2 Seguchi M., 2,3 It has shown 99.6% 4 Seguchi M.,
Stroke: Vascular and Interventional Neurology, Volume 3, Issue S2 , November 1, 2023. Rescue treatment with stenting, balloon angioplasty, and/or intraarterial thrombolysis or antiplatelets are often required to treat the underlying stenosis. Among these patients, 544 underwent rescue stenting, while 421 were control patients.
Important point: when there is diffuse subendocardial ischemia but no OMI, a wall motion abnormality will not necessarily be present. They agreed ischemia was likely in the setting of demand given DKA and infection. That this is all demand ischemia is unlikely. Lung exam showed diffuse B lines bilaterally. Aslanger's pattern.
Stroke: Vascular and Interventional Neurology, Volume 3, Issue S2 , November 1, 2023. Of note, patient had a with left cavernous‐ICA stent placement a month before the presentation and was noncompliant to antiplatelets. arterial dissection and or perforations). In the emergency department (ED), her NIHSS was 28. ED presentation was 2.5
2023 STS Coronary Conference Agenda gtrainyte Tue, 02/14/2023 - 09:13 Session titles and presenters are subject to change. Sabik III, MD, Cleveland, OH, USA Sigrid Sandner, MD, Vienna, Austria David Glineur, MD, PhD, Ottawa, ON, Canada Building an Advanced Coronary Surgery Program Day 1: Saturday, June 3, 2023 7:00 a.m. –
Stroke: Vascular and Interventional Neurology, Volume 3, Issue S2 , November 1, 2023. Herein, we describe a single‐step approach to deploy Neuroform Atlas stent (Stryker Neurovascular, Fremont, CA) which is a hybrid laser‐cut, nitinol self‐expanding stent without the need for ELW or lesion re‐access using MINI TREK RX (Abbott Vascular, Inc.,
ECG#1 Assessing ischemia on an ECG with wide QRS complexes (AIVR, ventricular pacing, BBB, etc) can be challenging. Many health care providers will simply not attempt to assess ischemia in the presence of a wide QRS. In the ECG above there are several features indicative of ongoing transmural ischemia. What do you think?
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chest pain relieved by rest. The baseline ECG is basically normal with no ischemia. In my opinion, I think it looks more like subendocardial ischemia.
The STD maximal in V1-V4 is diagnostic of acute transmural posterior wall ischemia, most likely due to posterior OMI. Subendocardial ischemia does not localize, and subendocardial ischemia presents with STD maximal in V5-6, II, and STE in aVR. Subendocardial ischemia does not localize. Finally the OMI was realized.
In any case, the ECG is diagnostic of severe ischemia and probably OMI. So this could be myocarditis but in my opinion needs an angiogram before making that diagnosis. == Dr. Nossen Comment/Interpretation: Evaluation of ischemia on an ECG can be very challenging. Concordant STE of 1 mm in just one lead or 2a.
Written by Jesse McLaren A 70 year old with prior MIs and stents to LAD and RCA presented to the emergency department with 2 weeks of increasing exertional chest pain radiating to the left arm, associated with nausea. But no ECG met STEMI criteria so the patient was referred to cardiology as Non-STEMI. Eur Heart J Digital Health 2024 5.
These tall T waves are associated with flattening ( straightening ) of the ST segment in the inferior leads — with slight S T elevation in leads V2-thru-V6 ( albeit not enough to qualify as a "STEMI" — Akbar et al, StatPearls, 2023 ). This point is discussed in detail in the March 24, 2023 post of Dr. Smith’s ECG Blog ).
The patient was referred immediately for cath which revealed RCA occlusion that was stented. Remember, in diffuse subendocardial ischemia with widespread ST-depression there may b e ST-E in lead s aVR and V1. There are well formed R-waves with good voltage/amplitude which is uncommon for ischemia. There is ST depression in V1.
The patient is female in her 80s with a medical hx of previous MI with PCI and stent placement. Are you confident there is no ischemia? Primary VT , and the VT with tachycardia is causing ischemia with chest discomfort (supply-demand mismatch/type 2 MI)? The last echocardiography 12 months ago showed HFmrEF.
Background Untreated multivessel disease (MVD) in acute myocardial infarction (AMI) has been linked to a higher risk of recurrent ischemia and death within one year. Databases were searched for relevant articles published before 10 November 2023. Pertinent data from the included studies were extracted and analyzed using RevMan v5.4.
I would expect TIMI-3 flow (normal flow, no persistent ischemia) with a culprit in the RCA (or possibly Circumflex). I would expect that a stent would be placed. The angiogram showed an open artery with 95% stenosis and thrombosis and it was stented. What would I expect the angiogram to show?
Stroke: Vascular and Interventional Neurology, Volume 3, Issue S2 , November 1, 2023. 5 ICSS‐ MRI study (International Carotid Stenting Study Magnetic Resonance Imaging Study), indicated that patients with periprocedural hemodynamic depression had decreased cerebral blood flow and increased the risk of new lesions in imaging.6
The pain will resolve and you will think the ischemia is gone when it is only hidden ! Just before 10 AM, the patient received a stent to the culprit OM. link] == MY Comment , by K EN G RAUER, MD ( 12/26/ 2023 ): == Interesting case by Dr. Frick — with superb illustration by him of cardiac cath findings!
Stroke: Vascular and Interventional Neurology, Volume 3, Issue S2 , November 1, 2023. Interventional approaches may include ECA‐ICA stenting with a covered stent or stent‐assisted coil embolization of the proximal stump.
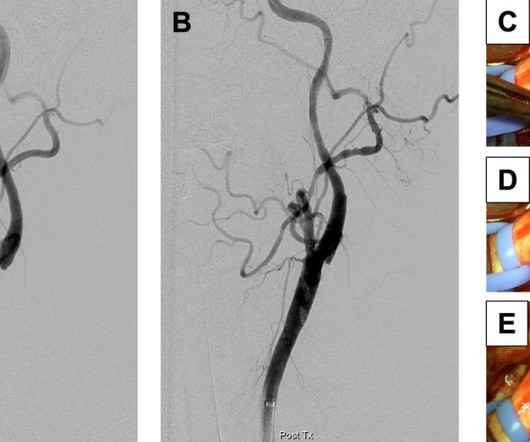
The patient’s angiogram should have been expedited, but the EKG change was not recognized as recurrence of transmural ischemia. RAO Caudal View Post PCI This is the RAO Caudal view after thrombectomy and stent placement. For more on use of Opiates with acute ischemic CP — See the January 6, 2023 post in Dr. Smith's ECG Blog ).
LAD: severe in-stent restenosis in the mid (80%) and distal (90%) segment and diffuse disease distally. Ramus intermedius: large, severe in-stent restenosis at the distal stent edge (90%) and severe de-novo stenosis at the ostial segment (90%). The pain did not resolve with NTG, and so he went to emergent angiography: 1.
I do not think this ECG is by itself diagnostic of OMI (full thickness, subepicardial ischemia ), b ut comparison to a previous might reveal this ECG as diagnostic of OMI. A single DES stent was placed, and the patient did well post-procedure. Abstract 556. You can't use absence of WMA to rule out need for emergent angiography!
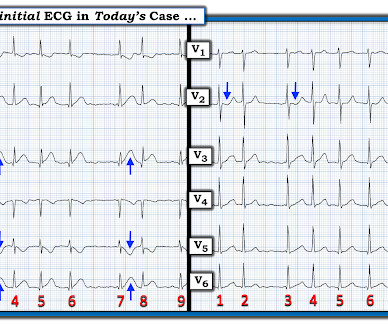
The patient, albeit very delayed was referred for angiography where a 99% stenosed pRCA was stented. For example — I've seen fast AFib be associated with significant ST elevation and depression that resolves after heart rate slows, and which was not a result of ischemia. Figure-1: The initial ECG in today's case. (
Prior ECG available on file from 2 months before: We do not know the clinical events happening during this ECG, but there is borderline tachycardia, PVCs, and likely some evidence of subendocardial ischemia with small STDs maximal in V5-6/II, slight reciprocal STE in aVR. Culprit lesion was reduced to 0% and stented.
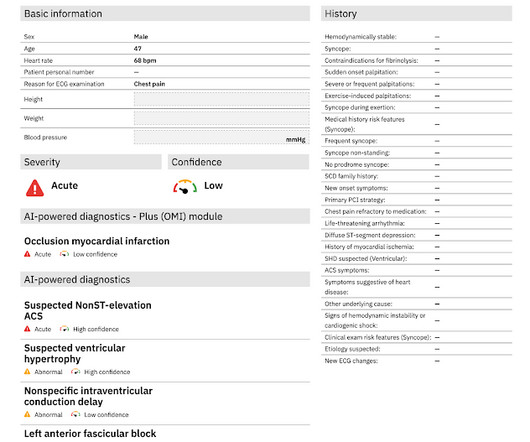
The ECG was incorrectly interpreted as no signs of ischemia. Artificial intelligence can be trained to recognize subtle OMI = My Comment by K EN G RAUER, MD ( 2/6 /2023 ): = The initial ECG in today's case was incorrectly interpreted as, "No signs of ischemia". No further ECG were ever recorded.
In other words, the inferior ST segments in the first ECG show more straightening which is more concerning for ischemia. The culprit lesion was opened and stented. Most notably the ST depression in the inferior leads is slightly more upsloping. The QoH interpretation however was the same for both ECGs.
Angiogram soon after (around 4 hrs after presentation) showed multi vessel CAD, with culprit lesion total occlusion of the first obtuse marginal branch (OM1), which was stented. My Comment by K EN G RAUER, MD ( 3/21 /2023 ): = Today's case provides one more example of an acute OMI not initially recognized by the On-Call interventionist.
All these factors, again, support an ECG diagnosis of LVH The patient was nonetheless taken for emergency angiography, and a 99% mid-LAD lesion was found and stented. However, the ST segments in patients with LVH may show significant variation over time in the absence of ischemia. 2023;Available from: [link] Am J Cardiol.
It was opened and stented. As a result — we do not know if ECG #2 represents a stable “baseline” tracing — or whether it might have been obtained during a period of ischemia in this patient with a history of known coronary disease. Formal bubble contrast echo: The estimated left ventricular ejection fraction 57%.
So the patient was taken for emergent cath, showing: Culprit artery: LAD (100% stenosis, TIMI 0) requiring thrombectomy and stent. EKG shown here: LAFB with no clear signs of OMI or ischemia. Queen of Hearts interpretation: Now the cardiologist considered it "STEMI"! No labs were performed. EKG and CT head were performed.
The diagnosis typically requires classic clinical features, with no evidence of obstructive coronary disease, and typical findings of ischemia on functional studies. But these are words you won’t find in the chest pain guidelines of 2023. This happens. But its rare!
Even though they were passed the 12 hour mark traditionally associated with reperfusion benefits, ongoing ischemia requires emergent angiogram On assessment, the patient appeared uncomfortable, leaning forward in his chair. ACS with refractory ischemia and electrical instability are indications for emergent cath regardless of the ECG!
The operator performed intravascular ultrasound and visualized acute plaque rupture with thrombus formation and placed a stent. There was reperfusion ischemia superimposed on benign T-wave inversion. He is very lucky that he spontaneously reperfused and was stented before he had the chance to re-occlude.
doi: 10.1136/jnis-2023-021243. Management The web can create a flow disturbance, potentiating local thrombus formation, which can embolize producing resulting in cerebral ischemia. Current treatment is with anti-thrombotics and/or anticoagulation.Lesser option is to alter the flow disturbance caused by the web (surgery or stent).
It was opened and stented. Compared to TTE from 7/3/24: the anterior regional wall motion abnormality is new and is consistent with ischemia/infarction in the LAD territory == MY Comment , by K EN G RAUER, MD ( 11/20 /2024 ): == There are several insightful aspects of today's case. The March 17, 2023 post — for PTA.
After stent deployment, we often see improvement in the ST-T within seconds or minutes. Here is the final angiogram following placement of a stent in the ostial RCA. 2:04 PM, post stent deployment You can see that even after complete restoration of flow, the ECG still looks terrible, V most of all. link] Jentzer, J. Kashou, A.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.









































Let's personalize your content