This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Here is his ED ECG at triage: Obvious high lateral OMI that does not quite meet STEMI criteria. This confirms that the pain was ischemia and is now resovled. For more on MINOCA — See My Comment in the November 16, 2023 post in Dr. Smith's ECG Blog ). He was given aspirin and sublingual nitro and the pain resolved.
Cath lab declined as it is not a STEMI." There is probably a trickle of flow which is why there is both subendocardial ischemia (ST depression) and early subepicardial ischemia (hyperacute T-waves). And now this finding is even formally endorsed as a "STEMI equivalent" in the 2022 ACC guidelines!!! It is a mass delusion.
The admission and discharge diagnosis both attributed the ECG changes and echo findings to ischemia. The biggest problem with STEMI criteria are false negatives – because this costs patient’s myocardium, with greater mortality and morbidity. baseline ECGs may fluctuate over time, and not necessarily represent dynamic ischemia 4.
mmm ECG Blog #193 — Reviews the concept of why the term “OMI” ( = O cclusion-based MI ) should replace the more familiar term STEMI — and — reviews the basics on how to predict the " culprit " artery. ECG Blog #271 — Reviews determination of the ST segment baseline ( with discussion of the entity of diffuse Subendocardial Ischemia).
The ECG shows severe ischemia, possibly posterior OMI. But cardiac arrest is a period of near zero flow in the coronary arteries and causes SEVERE ischemia. It takes time for that ischemia to resolve. Cardiac arrest #3: ST depression, Is it STEMI? And what do you want to do?
I sent this to the Queen of Hearts So the ECG is both STEMI negative and has no subtle diagnostic signs of occlusion. Non-STEMI guidelines call for “urgent/immediate invasive strategy is indicated in patients with NSTE-ACS who have refractory angina or hemodynamic or electrical instability,” regardless of ECG findings.[1]
Instead, pain is numbed and thus ischemia is obscured with opioids, excuses like hypertension are blamed, and unnecessary CT pulmonary angiograms are focused on. This patient does not show up in the STEMI registry, and the time to reperfusion will likely not be identified as the problem that it was.
Methods and Results Patients with confirmed ST elevation myocardial infarction (STEMI) treated by emergency medical services were included in this retrospective cohort analysis of the AVOID study. Greater severity of chest pain is presumed to be associated with a stronger likelihood of a true positive STEMI diagnosis. years old ± 13.7
These tall T waves are associated with flattening ( straightening ) of the ST segment in the inferior leads — with slight S T elevation in leads V2-thru-V6 ( albeit not enough to qualify as a "STEMI" — Akbar et al, StatPearls, 2023 ). This point is discussed in detail in the March 24, 2023 post of Dr. Smith’s ECG Blog ).
Acute Q waves are a marker of severe ischemia and a predictor for delayed reperfusion. This patient could have very easily been overlooked, both because the ECG was STEMI negative and because the Q waves were attributed to an “old infarct”. Fortunately, Dr. Cho was not looking for STEMI ECG criteria but for an acute coronary occlusion.
This was a machine read STEMI positive OMI. In this patient's case, the RV ischemia manifested as dramatic anterior hyperacute T waves. This degree of STE is a bit atypical for LAD ischemia. Written by Willy Frick A 50 year old man with no medical history presented with acute onset substernal chest pain. His ECG is shown below.
4,5] We have now formally studied this question: Emergency department Code STEMI patients with initial electrocardiogram labeled ‘normal’ by computer interpretation: a 7-year retrospective review.[6] have published a number of warnings about the previous reassuring studies.[4,5]
Important point: when there is diffuse subendocardial ischemia but no OMI, a wall motion abnormality will not necessarily be present. They agreed ischemia was likely in the setting of demand given DKA and infection. That this is all demand ischemia is unlikely. Lung exam showed diffuse B lines bilaterally. Aslanger's pattern.
Only very slight STE which does not meet STEMI criteria at this time. I am immediately worried that this OMI will not be understood, for many reasons including lack of sufficient STE for STEMI criteria, as well as the common misunderstanding of "no reciprocal findings" which is very common with this particular pattern.
The STD maximal in V1-V4 is diagnostic of acute transmural posterior wall ischemia, most likely due to posterior OMI. Subendocardial ischemia does not localize, and subendocardial ischemia presents with STD maximal in V5-6, II, and STE in aVR. It does not meet STEMI criteria. Subendocardial ischemia does not localize.
PEARL # 1: Although seeing an elevated Troponin would provide additional support for immediate cardiac catheterization — the clinical reality is that the initial Troponin reading will not always be elevated in patients with acute coronary occlusion ( See March 24, 2023 post in Dr. Smith's ECG Blog ).
would require the ST/S ratio to be 25% for diagnosis of STEMI in LVH. The physician was concerned about STEMI, but also worried that she was overreacting, with the potential that LVH was producing a "STEMI-mimic." Can you diagnose an ACO (STEMI) when you also have LVH? The criteria of Armstrong et al. References 1.
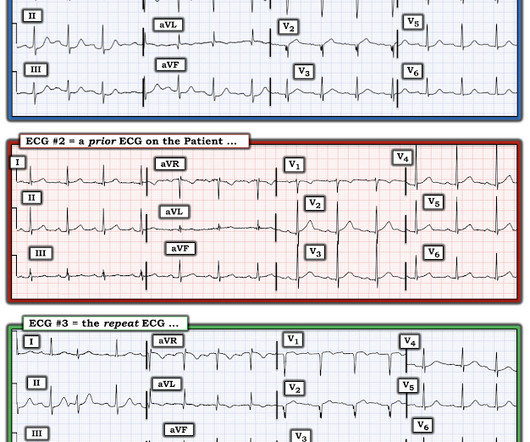
A prior ECG was available for comparison: Normal One might be tempted to interpret the ST depression as ischemia, but as Smith says, "when the QT is impossibly long, think of hypokalemia and a U-wave rather than T-wave." Is it STEMI? Instead — it commonly reflects ischemia from severe underlying coronary disease.
This suggests further severe ischemia. STEMI MINOCA versus NSTEMI MINOCA STEMI occurs in the presence of transmural ischaemia due to transient or persistent complete occlusion of the infarct-related coronary artery. This has resulted in an under-representation of STEMI MINOCA patients in the literature. From Gue at al.
Post Cath ECG: Obviously completing MI with LVA morphology, and STE that meets STEMI criteria (but pt is still diagnosed as "NSTEMI"). Smith : the profound persistent STE suggests either persistent occlusion or " no reflow " with persistent downstream ischemia. Long term outcome unknown but obviously bleak.
I would expect TIMI-3 flow (normal flow, no persistent ischemia) with a culprit in the RCA (or possibly Circumflex). Quiz : What percent of full blown STEMI have an open artery with normal flow at angiogram? It too is "normal" and you decide that this is not OMI or STEMI and you just decide to get troponins.
This is diagnostic of infero-posterior OMI, but it is falsely negative by STEMI criteria and with falsely negative posterior leads (though they do show mild ST elevation in V4R). They were less likely to have STEMI on ECG, and more likely to be initially diagnosed as non-ACS.
This blog post reviews the basics for predicting the " C ulprit" A rtery — as well as the importance of the term, " O MI" ( = O cclusion-based MI ) as an improvement from the outdated STEMI paradigm. ECG Blog #271 — Reviews determination of the ST segment baseline ( with discussion of the entity of diffuse Subendocardial Ischemia).
In any case, the ECG is diagnostic of severe ischemia and probably OMI. So this could be myocarditis but in my opinion needs an angiogram before making that diagnosis. == Dr. Nossen Comment/Interpretation: Evaluation of ischemia on an ECG can be very challenging. Concordant STE of 1 mm in just one lead or 2a.
It has been estimated that in the aggregate, they occur at a rate of about 3 per 1000 patients with acute MI, and most of these events occur in patients with STEMI. A mong patients with STEMI, ventricular septal rupture is the most common and free wall rupture is the least common.
Here, I do not see OMI (although the ECG is falsely STEMI positive with just over 1 mm STE in V1 and about 2.5 In the days before I learned to look for OMI, back when I was counting ST elevation boxes, I used to save ischemia for last.) I interpret tracings systematically in "real time" ( including my assessment for acute ischemia ).
The baseline ECG is basically normal with no ischemia. You can see in the lead-specific analysis that she "sees" the STD in V5, V5, and II, with STE in aVR as signs of "Not OMI", because subendocardial ischemia pattern is not the same as OMI. In my opinion, I think it looks more like subendocardial ischemia.
My interpretation was: RBBB with hyperacute T-waves in V4-V6 that are all but diagnostic of LAD occlusion vs. post ROSC ischemia. The patient had ROSC and maintained it. A 12-lead ECG was obtained: What do you think? Regional wall motion abnormality--apical anterior, mid anteroseptal, apical septal, and apical inferior akinesis.
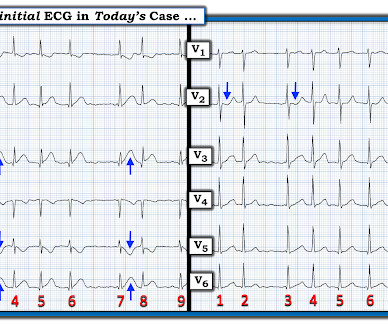
The precordial STD persists in severity from V4-V6, rather than being maximal in V1-V4 (as in posterior OMI), and so the ECG overall best fits the subendocardial ischemia pattern (diffuse supply/demand mismatch). A "STEMI alert" was called and soon cancelled.
The patient with no prior cardiac history presented in the middle of the night with acute chest pain, and had this ECG recorded during active pain: I did not see any ischemia on this electrocardiogram. This is a case I had quite a while back. There is a normal amount of ST elevation in the precordial leads.
There’s mild inferior ST elevation in III that doesn’t meet STEMI criteria, but it’s associated with ST depression in aVL and V2 that makes it diagnostic of infero-posterior Occlusion MI (from either RCA or circumflex)– accompanied by inferior Q waves of unknown age. Are there any signs of occlusion or reperfusion?
This blog post reviews the basics for predicting the " C ulprit" A rtery — as well as the importance of the term, " O MI" ( = O cclusion-based MI ) as an improvement from the outdated STEMI paradigm. ECG Blog #271 — Reviews determination of the ST segment baseline ( with discussion of the entity of diffuse Subendocardial Ischemia).
Learning Point: Concordant ST segment elevation can arise from profound ischemia triggered by ventricular tachycardia (VT), or it may represent an exaggerated basal ST change accompanying tachycardia. The patient rapidly regained consciousness, reporting no residual pain. A peak troponin level of 70 ng/L was observed.
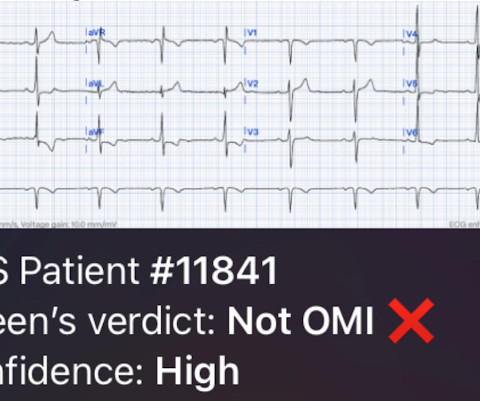
QOH versions 1 and 2 both say Not OMI, with high confidence, without any clinical context, despite the abnormal STE meeting STEMI criteria. That said — I did not interpret these differences as the result of acute ischemia. Of note, there is arguably terminal QRS distortion in V4-V6. Pericarditis maybe."
Looking at the location of ST elevation ( ie, in the inferior leads — and in V4,5,6 ) — and the location of ST depression ( ie, in leads I,aVL; V1,V2 ) — this ECG picture suggests an ongoing acute infero - postero - lateral STEMI. What is S hark F in M orphology ? Cardiopulmonary resuscitation was promptly started — but was unsuccessful.
I knew that, if the patient had presented with chest discomfort, that this ECG is diagnostic of inferior posterior OMI, even though it is not a STEMI. In subendocardial ischemia, cath lab is indicated if the pain persists in spite of medical therapy (aspirin, anticoagulant, IV nitro). At 100 minutes, the above ECG was recorded.
There is normal R-wave progression in the precordial leads with no evidence of ischemia. Troponin T peaked at 2074 ng/L (very high, typical of OMI/STEMI). Here the image quality is enhanced using the PM Cardio app. What do you think? The presenting ECG shows SR with narrow QRS complexes. The LV EF was 57% at formal echo.
At 2111, the troponin I peaked at 12.252 ng/mL (this is in the range of STEMI patients, quite high). The patient’s angiogram should have been expedited, but the EKG change was not recognized as recurrence of transmural ischemia. For more on use of Opiates with acute ischemic CP — See the January 6, 2023 post in Dr. Smith's ECG Blog ).
Code STEMI was activated by the ED physician based on the diagnostic ECG for LAD OMI in ventricular paced rhythm. This was several months after the 2022 ACC Guidelines adding modified Sgarbossa criteria as a STEMI equivalent in ventricular paced rhythm). LAFB, atrial flutter, anterolateral STEMI(+) OMI. Limkakeng AT.
KEY Point: In areas of the heart where an acute STEMI produces ST elevation — reperfusion T waves ( that develop after the "culprit" artery reopens ) will appear as T wave inversion. In 2023 — it should be EASY to locate and transmit previous ECGs for comparison from established patients.
The Queen of Hearts correctly says: Smith : Why is this ECG which manifests so much ST Elevation NOT a STEMI (even if it were a 60 year old with chest pain)? Physician interpretation: "No STEMI." Physician: "No STEMI." Cardiologist interpretation: "Technically does not meet STEMI criteria but concerning for ischemia."
Inferior ST Depression does NOT mean there is inferior subendocardial ischemia; it is generally reciprocal to high lateral (aVL) subepicardial ischemia (OMI/STEMI) == MY Comment by K EN G RAUER, MD ( 2/10/2023 ): == There are certain patterns in ECG interpretation that experienced providers are able to immediately recognize.
I do not think this ECG is by itself diagnostic of OMI (full thickness, subepicardial ischemia ), b ut comparison to a previous might reveal this ECG as diagnostic of OMI. Immediate and early percutaneous coronary intervention in very high-risk and high-risk Non-STEMI patients. Lupu L, et al. mg/dL, K 3.5 Abstract 556.
Notice that much of the dark blue is concentrated on the QRS (R-wave); the QRS is totally ignored in the STEMI paradigm!! In my opinion — the problem is not giving morphine, but rather the inability to recognize acute ECG changes when millimeter-based stemi criteria are not attained. aVL has a lot of dark blue also, as does lead I.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
















































Let's personalize your content