This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Late-breaking second year results from the PROMISE II trial showed that the LimFlow system achieved strong outcomes for avoiding amputations and promoting limb salvage among “no-option” patients with chronic limb-threatening ischemia (CLTI). LimFlow gained FDA approval in September 2023, and was soon acquired by Inari Medical for up to $415M.
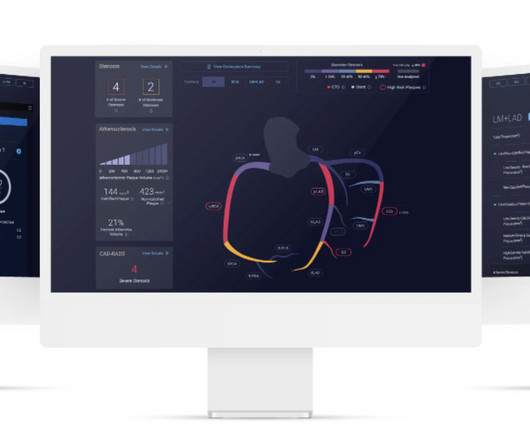
Food and Drug Administration ( FDA )-cleared Cleerly ISCHEMIA software device applied to a non-invasive coronary CT angiogram ( CCTA ) can be billed using the new Category I CPT code 75580. Prior studies have demonstrated the independent and incremental benefit of Cleerly ISCHEMIA applied to CCTA beyond traditional assessment.
As the medical community delves deeper into the intricacies of ANOCA, the study provides a compelling narrative for clinicians and researchers alike, aiming to decipher the complexities of myocardial bridges and their role in exercise-induced ischemia. Original article: Sinha A et al. Circ Cardiovasc Interv.
This confirms that the pain was ischemia and is now resovled. For more on MINOCA — See My Comment in the November 16, 2023 post in Dr. Smith's ECG Blog ). The cardiology fellow agreed with plan for emergent cath and escorted the patient to the cath lab. The i nitial hs troponin I returned 75%.
The study describes the validation of Cleerly's artificial intelligence-guided quantitative coronary CT angiography (AI-QCT) ISCHEMIA technology for diagnostic accuracy and prognostic risk stratification. High Diagnostic Accuracy of AI-ISCHEMIA in Comparison to PET, FFR-CT, SPECT, and Invasive FFR: A Pacific Substudy. 2024.01.007.
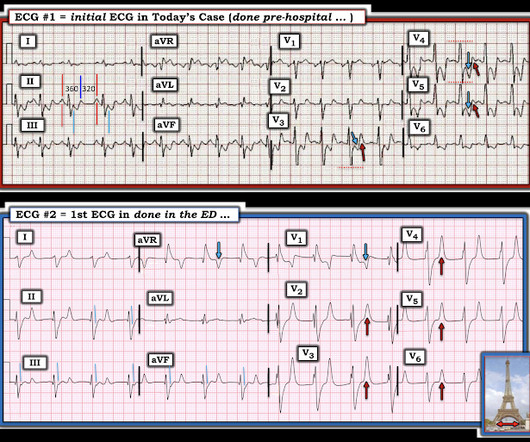
The ECG shows severe ischemia, possibly posterior OMI. But cardiac arrest is a period of near zero flow in the coronary arteries and causes SEVERE ischemia. It takes time for that ischemia to resolve. The patient was brought to the ED and had this ECG recorded: What do you think? And what do you want to do?
High Diagnostic Accuracy Of AI-Ischemia in Comparison To PET, FFR-CT, SPECT, and Invasive FFR: A PACIFIC Sub-Study. Presented at the American College of Cardiology Annual Scientific Meeting New Orleans LA 2023. Presented at the Society of Cardiovascular Computed Tomography Annual Scientific Meeting Boston MA 2023.
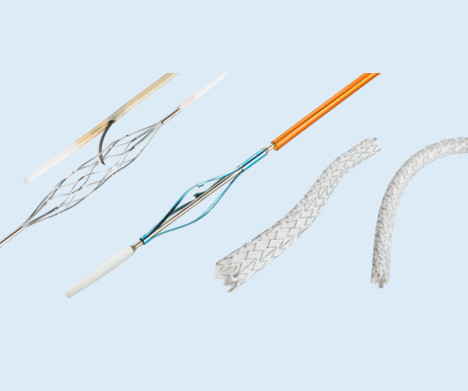
The Freesolve BTK RMS is designed for individuals suffering from chronic limb-threatening ischemia (CLTI). Updated estimates for the burden of chronic limb-threatening ischemia in the Medicare population, Journal of Vascular Surgery, Volume 77, Issue 6, 2023, 1760-1775 2 Seguchi M., 4 Seguchi M.,
ii to show blood flow through the heart muscle and evaluate the presence, extent and degree of myocardial ischemia or infarction. 2023 Oct, 82 (16) 15981610. Around 6 million MPI procedures are undertaken each year in theU.S. Flyrcado is now available in selectU.S.markets. Click here to learn more about Flyrcado. link] ii Miller, R.
2023 STS Coronary Conference Agenda gtrainyte Tue, 02/14/2023 - 09:13 Session titles and presenters are subject to change. Sabik III, MD, Cleveland, OH, USA Sigrid Sandner, MD, Vienna, Austria David Glineur, MD, PhD, Ottawa, ON, Canada Building an Advanced Coronary Surgery Program Day 1: Saturday, June 3, 2023 7:00 a.m. –
Important point: when there is diffuse subendocardial ischemia but no OMI, a wall motion abnormality will not necessarily be present. They agreed ischemia was likely in the setting of demand given DKA and infection. That this is all demand ischemia is unlikely. Lung exam showed diffuse B lines bilaterally. Aslanger's pattern.
ECG Blog #184 — illustrates the "magical" mirror-image opposite relationship with acute ischemia between lead III and lead aVL ( featured in Audio Pearl #2 in this blog post ). ECG Blog #271 — Reviews determination of the ST segment baseline ( with discussion of the entity of diffuse Subendocardial Ischemia).
Stroke: Vascular and Interventional Neurology, Volume 3, Issue S2 , November 1, 2023. IntroductionAcute spinal cord ischemia syndrome (ASCIS) is a rare disease that is thought to comprise roughly only 1.2% of all strokes [1, 2]. Due to the scarcity of these events, the patient outcomes are unclear.
The ECG does not show any definite signs of ischemia. This combination is often extremely effective for maintaining good longterm outcome ( Lanza and Shimokawa — Eur Cardiol 18: e38, 2023 ). The patient presented due to chest pain that was typical in nature, retrosternal and radiating to the left arm and neck.
6 This novel study marks a significant milestone in the field, evaluating the effectiveness of FFR CT in detecting ischemia-producing coronary stenosis in patients with severe PAD. Diagnosis and treatment of ischemia-producing coronary stenoses improves 5-year survival of patients undergoing major vascular surgery.” 2024, [link].
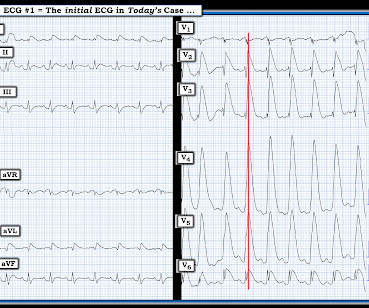
My written interpretation on a tracing such as this one would read, "Marked LVH and 'strain' and/or ischemia — with need for clinical correlation." BOTTOM LINE: ECG changes of LV "strain" and/or ischemia that we see on today's initial ECG — were not present 9 years earlier. Please see ECG Blog #73 for additional details ).
The STD maximal in V1-V4 is diagnostic of acute transmural posterior wall ischemia, most likely due to posterior OMI. Subendocardial ischemia does not localize, and subendocardial ischemia presents with STD maximal in V5-6, II, and STE in aVR. Subendocardial ischemia does not localize.
The first task when assessing a wide complex QRS for ischemia is to identify the end of the QRS. The ST segment changes are compatible with severe subendocardial ischemia which can be caused by type I MI from ACS or potentially from type II MI (non-obstructive coronary artery disease with supply/demand mismatch). What do you think?
Shark Fin" ST segment elevation is most often a sign of severe transmural ischemia that results from acute coronary occlusion. As a result — the boundary between the end of the QRS complex and the beginning of the ST segment becomes indistinguishable in those leads showing marked ST elevation or depression.
A prior ECG was available for comparison: Normal One might be tempted to interpret the ST depression as ischemia, but as Smith says, "when the QT is impossibly long, think of hypokalemia and a U-wave rather than T-wave." QUESTION #2: If it were not for the markedly prolonged QTc — Wouldn't ECG #1 look like diffuse subendocardial ischemia?
Instead, pain is numbed and thus ischemia is obscured with opioids, excuses like hypertension are blamed, and unnecessary CT pulmonary angiograms are focused on. Figure-1: The de Winter T Wave Pattern , as first described by Robbert J. de Winter et al in N Engl J Med 359:2071-2073, 2008.
ECG#1 Assessing ischemia on an ECG with wide QRS complexes (AIVR, ventricular pacing, BBB, etc) can be challenging. Many health care providers will simply not attempt to assess ischemia in the presence of a wide QRS. In the ECG above there are several features indicative of ongoing transmural ischemia. What do you think?
PEARL # 1: Although seeing an elevated Troponin would provide additional support for immediate cardiac catheterization — the clinical reality is that the initial Troponin reading will not always be elevated in patients with acute coronary occlusion ( See March 24, 2023 post in Dr. Smith's ECG Blog ).
As a result, the ST elevation ( with especially tall, peaked T wave in lead V2) — is not indication of acute ischemia. As suggested by Figure-4 below in the ADDENDUM — assessment of the ST-T waves in leads V2,V3 and V5,V6 — is consistent with ischemia and / or LV "strain".
Results revealed ischemia in one cardiac territory in 80% of patients, two territories in 17%, and three territories in 2%. The investigators concluded that in patients with stable angina and minimal medication, confirmed ischemia, and randomized to PCI, the procedure led to better angina outcomes compared to the placebo. N Engl J Med.
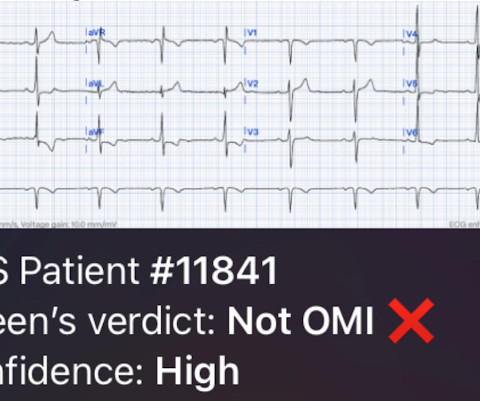
The baseline ECG is basically normal with no ischemia. You can see in the lead-specific analysis that she "sees" the STD in V5, V5, and II, with STE in aVR as signs of "Not OMI", because subendocardial ischemia pattern is not the same as OMI. In my opinion, I think it looks more like subendocardial ischemia.
In this patient's case, the RV ischemia manifested as dramatic anterior hyperacute T waves. This degree of STE is a bit atypical for LAD ischemia. Remember that the RV is the most anterior chamber. Here is a transverse image of a CT showing this. A few clues that might have suggested this are: There is marked STE in V1.
Critical limb-threatening ischemia (CLTI) represents the end stage of peripheral artery disease (PAD), when poor circulation due to blockages in the arteries causes symptoms including numbness, sores that will not heal, gangrene, and extreme pain. When we save a limb, we save a life.
In any case, the ECG is diagnostic of severe ischemia and probably OMI. So this could be myocarditis but in my opinion needs an angiogram before making that diagnosis. == Dr. Nossen Comment/Interpretation: Evaluation of ischemia on an ECG can be very challenging. Concordant STE of 1 mm in just one lead or 2a.
In the days before I learned to look for OMI, back when I was counting ST elevation boxes, I used to save ischemia for last.) I interpret tracings systematically in "real time" ( including my assessment for acute ischemia ). The January 15, 2023 post ( LA-LL reversal; Lead V1,V2 ). The May 13, 2023 post ( LA-RA reversal ).
These tall T waves are associated with flattening ( straightening ) of the ST segment in the inferior leads — with slight S T elevation in leads V2-thru-V6 ( albeit not enough to qualify as a "STEMI" — Akbar et al, StatPearls, 2023 ). This point is discussed in detail in the March 24, 2023 post of Dr. Smith’s ECG Blog ).
Remember, in diffuse subendocardial ischemia with widespread ST-depression there may b e ST-E in lead s aVR and V1. There are well formed R-waves with good voltage/amplitude which is uncommon for ischemia. The ECG does not show any signs of ischemia. True Positive ECG#2 : Also sinus rhythm. There is ST depression in V1.
It should be kept in mind that on occasions, beta-one agonist can result in increased ventricular ectopy e.g., in severe myocardial ischemia (by increasing myocardial demand), or sometimes with congenital long-QT syndrome. Smith, this can be accomplished by either using beta-one agonists or temporary transvenous pacing.
The precordial STD persists in severity from V4-V6, rather than being maximal in V1-V4 (as in posterior OMI), and so the ECG overall best fits the subendocardial ischemia pattern (diffuse supply/demand mismatch). Instead, diffuse subendocardial ischemia may be present with ST depression in only 7 or 8 leads.
Are you confident there is no ischemia? Primary VT , and the VT with tachycardia is causing ischemia with chest discomfort (supply-demand mismatch/type 2 MI)? Ischemia from ACS causing the chest discomfort, with VT another consequence (or coincidence)? Do you agree with this strategy? How can you better assess the ST segments?
This proves effective treatment of the recurrent ischemia. The patient had no further symptoms of ischemia. EKG 3 is diagnostic for developing re-occlusion, and EKG 4 proves that the nitrates relieved the ischemia. = This proves effective treatment of the recurrent ischemia." Here was her final EKG prior to discharge.
Here is the only prehospital 12-lead: Sinus tachycardia, somewhat wide QRS, Ischemia Here is the first ED ECG: What is the rhythm here? He was resuscitated into a perfusing rhythm. He went in and out of arrest until arrival at the ED. Instead — these peaked deflections represent part of the ST-T wave!
ECG Blog #184 — illustrates the "magical" mirror-image opposite relationship with acute ischemia between lead III and lead aVL ( featured in Audio Pearl #2 in this blog post ). ECG Blog #271 — Reviews determination of the ST segment baseline ( with discussion of the entity of diffuse Subendocardial Ischemia).
PMID: 11723026. == MY Comment , by K EN G RAUER, MD ( 10/23 /2023 ): == The various forms of electrical alternans are frequently misunderstood, if not completely unnoticed. Alternation in ST segment appearance ( or in the amount of ST elevation or depression ) — is often linked to ischemia. Circulation. 2001 Nov 27;104(22):2722-7.
5] Back to the case The patient had serial ECGs over the next hour with no significant change: The first troponin came back at 1,400 ng/L (normal <26 in males and <16 in females), confirming MI – and the patient’s refractory ischemia indicated this was an Occlusion MI. Eur Heart J Digital Health 2024 5. McLaren and Smith.
When I was shown this ECG, I said it looks like such widespread ischemia that is might be a left main occlusion, or LM ischemia plus circumflex occlusion (high lateral and posterior OMI). There is STE in aVR. Thus, there is high lateral OMI with diffuse ST depression. Moreover, left main occlusion often presents near death.
Osborn waves have been reported with hypercalcemia, brain injury, subarachnoid hemorrhage, Brugada syndrome, cardiac arrest from VFib — and — severe, acute ischemia resulting in acute MI ( See My Comment in the November 22, 2019 post on Dr. Smith’s Blog ). Rituparna et al — as well as Chauhan and Brahma ( Int.
The admission and discharge diagnosis both attributed the ECG changes and echo findings to ischemia. baseline ECGs may fluctuate over time, and not necessarily represent dynamic ischemia 4. Below is the discharge ECG, which showed the baseline ECG without any reperfusion T wave inversion. Take home 1. I'd add the following to Dr.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.










































Let's personalize your content