This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Coronaryarterydisease is caused by the retention of a cholesterol particle in the artery wall. On the far end of that line is type two diabetes. On the far end of that line is type two diabetes. We also know that WHEN you get type 2 diabetes makes a huge difference. Let me be 100% clear, however.
A common feedback I get is that people with existing coronaryarterydisease feel like it doesn’t apply to them. Arguably, applying the principles of prevention offers more bang for buck in the short term for people WITH coronaryarterydisease than those without coronaryarterydisease.
Background:Clinical trials have demonstrated that sodium-glucose cotransporter-2 inhibitors (SGLT2i) and glucagon-like peptide-1 receptor agonists (GLP1RA) reduce cardiovascular (CV) risk in patients (pts) with type 2 diabetes (T2D) with or at high risk for CV disease. 1.04, P=0.3). 0.98, P=0.025).Conclusions:Among
But the goal in this instance is to die after a long and healthy life ‘ with ’ coronaryarterydisease rather than ‘ from ’ coronaryarterydisease. However, the chances of dying from heart disease are directly proportional to the amount of plaque in your coronaryarteries.
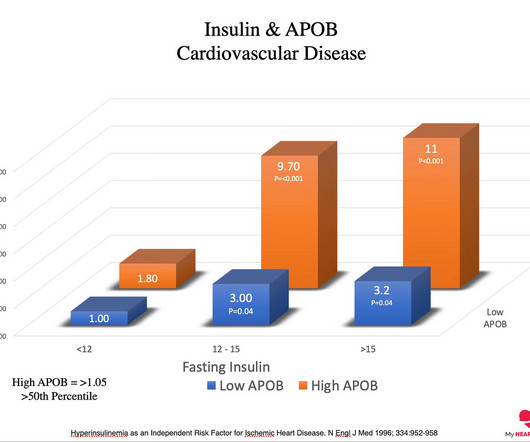
Excess visceral fat results in a higher risk of insulin resistance, which is the precursor state to diabetes. In the setting of insulin resistance, a higher ApoB concentration increases the risk of cardiovascular disease dramatically. Relationship of BMI and Risk Of Diabetes. You put their diabetes into remission.
Between 2020 and 2023, the rates of obesity dropped by about 2% 2. Inflammation is a key driver of heart disease, specifically coronaryarterydisease. Sci Rep 13 , 20998 (2023). Semaglutide and Cardiovascular Outcomes in Obesity without Diabetes. 2023 Dec 14;389(24):2221-2232. Inflammation.
This study aims to investigate the relationship between sdLDLC level and PP in patients with stable coronaryartery disease.MethodsWe conducted a retrospective analysis of 146 lesions in 86 patients by repeat intravascular ultrasound examinations from January 2020 to May 2023. P<0.001).
Atherosclerotic cardiovascular disease (ASCVD), caused by plaque buildup in arterial walls, is one of the leading causes of disability and death worldwide.1,2 1,2 ASCVD causes or contributes to conditions that include coronaryarterydisease (CAD), cerebrovascular disease, and peripheral vascular disease (inclusive of aortic aneurysm).3
Stroke: Vascular and Interventional Neurology, Volume 3, Issue S2 , November 1, 2023. Type 2 Diabetes Mellitus (T2DM) is a rapidly growing global health problem with increasing prevalence. Type 2 Diabetes Mellitus (T2DM) is a rapidly growing global health problem with increasing prevalence.
Stroke: Vascular and Interventional Neurology, Volume 3, Issue S2 , November 1, 2023. IntroductionThere is a higher prevalence of diabetes mellitus type 2 in Hispanics as compared to other ethnic groups in the United States. vs 72, p<0.001) compared to patients who did not have poorly controlled diabetes. or greater.
A 56 year old male with a history of diabetes, dyslipidemia, hypertension, and coronaryarterydisease presented to the emergency department with sudden onset weakness, fatigue, lethargy, and confusion. For more on use of Opiates with acute ischemic CP — See the January 6, 2023 post in Dr. Smith's ECG Blog ).
An elevated Lp(a) is a common genetic factor that is independently and causally related to premature coronaryarterydisease. The occurrence of disease in this instance is probabilistic, not deterministic. An elevated Lp(a) does increase the risk of early cardiovascular disease, but that risk is not set in stone.
Written by Magnus Nossen The patient in today's case is a male in his 70s with hypertension and type II diabetes mellitus. The ST segment changes are compatible with severe subendocardial ischemia which can be caused by type I MI from ACS or potentially from type II MI (non-obstructive coronaryarterydisease with supply/demand mismatch).
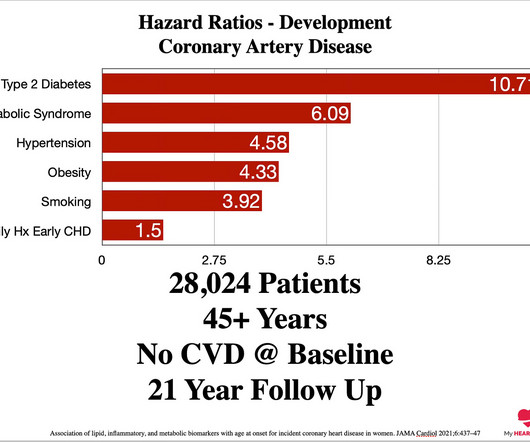
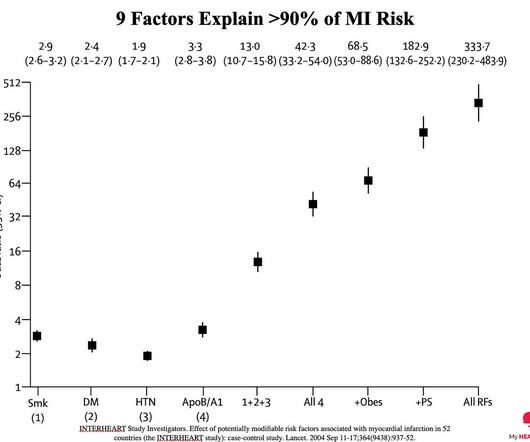
If you take someone who has multiple risk factors for heart disease, including diabetes, smoking, abnormal cholesterol and high blood pressure, they have a 42 times higher risk of a heart attack compared to someone who does not have any of these factors. 24% increased risk of coronaryarterydisease.
Pulse was 115, BP 140/65, and afebrile He was found to have cellulitis and to be in diabetic ketoacidosis, with bicarb of 14, pH of 2.27, glucose of 381, anion gap of 18, and lactate of 2.2 One would expect that the angiogram would show open arteries with normal TIMI-3 flow and culprit lesions. Normal left ventricular wall thickness.
Stroke: Vascular and Interventional Neurology, Volume 3, Issue S2 , November 1, 2023. Median LDL was higher (94 vs 67, p=0.01) and there was a higher rate of diabetes (55.2% IntroductionThe risk of tandem occlusion treatment in the setting of intravenous thrombolysis is unclear. vs 26.6%, p=0.01).
Stroke: Vascular and Interventional Neurology, Volume 3, Issue S2 , November 1, 2023. IntroductionSubarachnoid Hemorrhage (SAH) is the leading cause of morbidity and mortality in stroke patients, associated with severe neurological, infectious, and thromboembolic complications. x) from 2016‐2019.
Diamond and Forrester accomplished this by first establishing the prevalence of coronaryarterydisease based on how clinically likely patients with chest pain symptoms were found to have coronarydisease based on a coronary angiogram. years of age, P <0.001), cerebral or peripheral arterydisease (6.2%
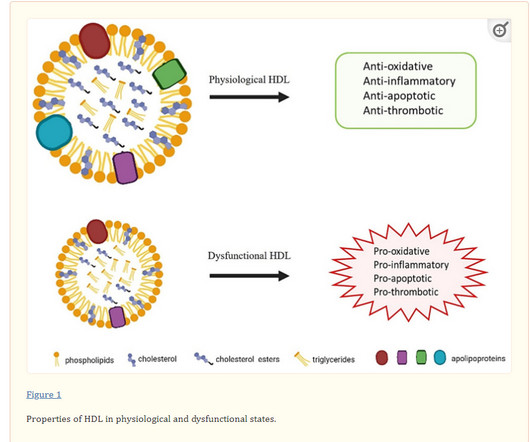
Types of HDL dysfunction : A combination of obesity & diabetes has high chance of pushing this molecule into bad times. Glycolysation of HDL Diabetics results in systemic glycation of all cells or whatever molecule the blood bathes in. Sounds more ominous than LDL is it not ?) As of now, there is no practical tests to know it.
Stroke: Vascular and Interventional Neurology, Volume 3, Issue S2 , November 1, 2023. They also had a higher prevalence of diabetes (32.43% and 32.82% vs 28.42%), dyslipidemia (44.57% and 44.81% vs 41.41%), obesity (13.19% and 13.64% vs 12.03%), prior TIA/ischemic stroke (6.46% and 6.52&
Stroke: Vascular and Interventional Neurology, Volume 3, Issue S2 , November 1, 2023. IntroductionMycotic aneurysms of paraspinal arteries are a rare finding. Furthermore, knowledge regarding the management of paraspinal mycotic aneurysms and the efficacy of endovascular repair of these lesions is scarce.⁴MethodsWe
Salvatore Carbone, PhD: First, I’d like to point out that obesity is a major risk factor for cardiometabolic disease. There are significant data that show that if you have obesity, you have a high risk of developing coronary heart disease, heart failure, type 2 diabetes (T2D) or risk factors such as hypertension and dyslipidemia. [1]
The current analysis pools data from 16 studies conducted between January 2000 and May 2023, evaluating hypertension incidence in 1,044,035 people from six countries who did not have a prior history of high blood pressure over a median follow-up of five years (follow-up ranged from 2.4 to 18 years).
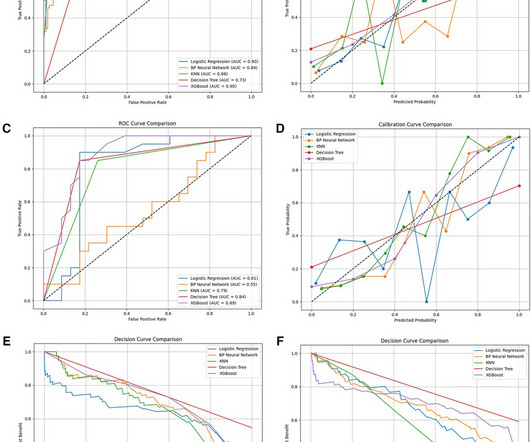
For external validation, 143 patients who were admitted between February and June 2023 from a different associated hospital in Lu'an City were also used.ResultsThe XGBoost model demonstrated the most accurate prediction performance out of the five machine learning techniques.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
























Let's personalize your content