This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
For example, considering whatever symptoms that the patient may have had ( ie, chestpain, palpitations, shortness of breath, etc. ) — what this might mean in view of the ECG we are looking at. To quote Dr. Stephen Smith: "The worst riskfactor for a bad outcome in acute MI is young age."
By Magnus Nossen This ECG is from a young man with no riskfactors for CAD, he presented with chestpain. The patient is a young adult male with chestpain. The chestpain was described as pressure like and radiation to both arms and the jaw. How would you assess this ECG?
Healthy male under 25 years old with a pretty good story for acute onset crushing chestpain relieved with nitro. Aggressive riskfactor modification. PEARL: Most patients who present with new chestpain + ECG changes + positive troponin — will not need Cardiac MRI. No pericardial effusion on ultrasound."
Circulation: Genomic and Precision Medicine, Volume 16, Issue 5 , Page 442-451, October 1, 2023. Background:Patients with de novo chestpain, referred for evaluation of possible coronary artery disease (CAD), frequently have an absence of CAD resulting in millions of tests not having any clinical impact.
No prior exertional complaints of chestpain, dizziness, lightheadedness, or undue shortness of breath. He denied headache or neck pain associated with exertion. I sent this ECG to Dr. Smith, with the only information that it is a 17 year old with chestpain. 24 yo woman with chestpain: Is this STEMI?
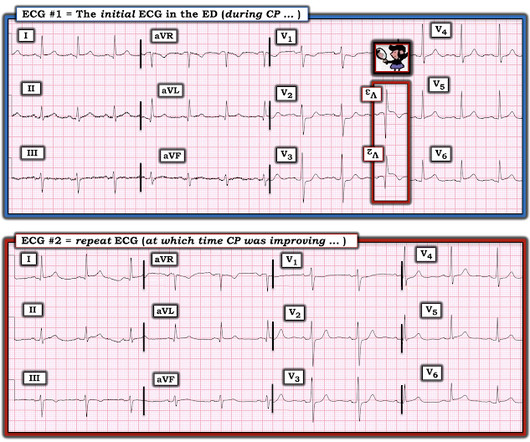
A 50-something with no previous cardiac history and no riskfactors presented to the ED with acute chestpain (pressure) that radiated to the left arm. The Scenario in Today's Case: We are told that the patient in today's case noted a reduction in chestpain at the time ECG #2 was recorded.
Submitted by Ali Khan MD and James Mantas MD, MS, written by Pendell Meyers A man in his 50s with history of diabetes, hypertension, and tobacco use presented to the ED with 24 hours of worsening left sided chestpain radiating to the back, characterized as squeezing and pinching, associated with shortness of breath.
milla1cf Wed, 12/13/2023 - 10:24 December 13, 2023 — A new artificial intelligence (AI) model designed by Scripps Research scientists could help clinicians better screen patients for atrial fibrillation (or AFib)—an irregular, fast heartbeat that is associated with stroke and heart failure.
On the second morning of his admission, he developed 10/10 chestpain and some diaphoresis after breakfast. The patient was given opiates which improved his chestpain to 7/10. The consulting cardiologist wrote in their note: “Could be cardiac chestpain. She is usually incredibly good at recognizing them!
Stroke: Vascular and Interventional Neurology, Volume 3, Issue S2 , November 1, 2023. IntroductionPatients with cognitive impairment often have a history of cardiovascular disease (CVD) or multiple cardiovascular riskfactors (CRFs) such as hypertension, obesity, and hypercholesterolemia. MBq/kg dose of FDG.
Riskfactors such as high blood pressure, smoking, and inactivity are important because the longer you are exposed to them, the higher the odds you will develop coronary artery disease sooner in life. And, by extension, have a higher risk of a heart attack. But not everyone with riskfactors develops early heart disease.
More than 8 million Americans visit hospital emergency departments experiencing chestpain every year. In June 2023, the U.S. “In the future, patients with coronary inflammation can be identified by the CaRi-Heart technology and treated by our FDA -approved LODOCO 0.5 mg tablets.”
He denied chestpain or shortness of breath. In the clinical context of weakness and fever, without chestpain or shortness of breath, the likelihood of Brugada pattern is obviously much higher. Today's patient presented with acute weakness, syncope and fever, but no chestpain or shortness of breath.
This means that at every age, the probability a man complaining of chestpain has significant underlying coronary disease as a cause of this chestpain is much higher than a woman complaining of chestpain. Women also had more cardiovascular riskfactors, including hypertension (66.6%
As discussed in detail in ECG Blog #228 — this seemingly qualifies as a “ Silent ” MI ( Approximately half of those MIs not accompanied by CP — have some other associated symptom such as syncope, which substitutes as a “chestpain equivalent” ). Longterm prognosis of patients with MINOCA clearly depends on the underlying etiology.
Stroke: Vascular and Interventional Neurology, Volume 3, Issue S2 , November 1, 2023. Riskfactors such as smoking, chronic kidney disease, and aging can contribute to plaque formation. Riskfactors such as smoking, chronic kidney disease, and aging can contribute to plaque formation.
Getty Images milla1cf Fri, 12/08/2023 - 08:17 December 8, 2023 — The American College of Cardiology (ACC) and the American Heart Association (AHA), along with several other leading medical associations, have issued a new guideline for preventing and optimally managing atrial fibrillation (AFib).
link] A 62 year old man with a history of hypertension, type 2 diabetes mellitus, and carotid artery stenosis called 911 at 9:30 in the morning with complaint of chestpain. He described it as "10/10" intensity, radiating across his chest from right to left. This is written by Willy Frick, an amazing cardiology fellow in St.
24 will focus on the following three current guideline updates: American College of Cardiology (ACC)/American Heart Association (AHA) Guidelines 2023 Atrial Fibrillation Guideline - Pharmacology II: Strokes vs. Bleeds, What Do the Guidelines Tell Us About Practical Management in A-fib? The Guidelines Sessions at ACC.24
A 70-something female with no previous cardiac history presented with acute chestpain. She awoke from sleep last night around 4:45 AM (3 hours prior to arrival) with pain that originated in her mid back. She stated the pain was achy/crampy. Over the course of the next hour, this pain turned into a pressure in her chest.
Case "Male, 43yo, come to ED with Epigastric Pain started 3 hours ago. RiskFactors: High Cholesterol. My Comment by K EN G RAUER, MD ( 3/21 /2023 ): = Today's case provides one more example of an acute OMI not initially recognized by the On-Call interventionist. Vitals Signs: Normal." Teaching is rewarding!
The patient contacted EMS after a few hours of chestpain that started 5:30 AM. The pain was described as 6/10 radiating to the right shoulder. The chestpain was described as both sharp and pressure like. There is slight ST depression in lateral chest leads V4,V5,V6 — but I thought this to be nonspecific.
Diagnosis : Atrial flutter with 1:1 conduction, with fast AV conduction made possible by sympathetic drive of exercise On arrival, we obtained another 12-lead: Unremarkable Further history: One month history of shortness of breath on exertion, denies palpitations, chestpain, orthopnea, leg swelling.
days of chestpain that started as substernal and crushing in nature awakening him from sleep and occasionally traveling to right side of neck. The pain was described as constant, worse with deep inspiration and physical activity, sometimes sharp. He reported 1.5 World J Pediatr. 2021 Aug;17(4):335-340. Epub 2021 May 20.
Written by Willy Frick A 51 year old man with hypertension presented with three hours of acute onset, severe midsternal chestpain associated with two episodes of nausea and vomiting. or 2) Inferior and lateral OMI that is beginning to reperfuse, even though the patient still has chestpain? ECG 1 What do you think?
A 50-something male presented to triage with chestpain for one day. A Chest X-ray showed infiltrates. Thus, another etiology of chestpain is found, and the fever suggests "fever-induced Brugada." The presenting complaint noted at Triage was, "a 50yo man with chestpain!" The temperature was 39.5
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




























Let's personalize your content