This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
2 middle aged males presented with chestpain. Which had the more severe chestpain at the time of the ECG? Patient 2 at the bottom with a very subtle OMI complained of 10/10 chestpain at the time the ECG was recorded. 414 patients were included in the analysis.
For example, considering whatever symptoms that the patient may have had ( ie, chestpain, palpitations, shortness of breath, etc. ) — what this might mean in view of the ECG we are looking at. STEP #2 = Clinical Impression — in which we correlate our assessment that we made in Step #1 to the clinical situation at hand.
By Magnus Nossen This ECG is from a young man with no risk factors for CAD, he presented with chestpain. The patient is a young adult male with chestpain. The chestpain was described as pressure like and radiation to both arms and the jaw. How would you assess this ECG? What is your next step?
Written by Jesse McLaren A 45 year old presented with two weeks of recurring non-exertional chestpain, now constant for an hour. Because of the ECG changes in a patient with chestpain, and with inferolateral hypokinesis on POCUS, the cath lab was activated. Below is old and then new ECG (old on top; new below).
Written by Magnus Nossen with Edits by Grauer and Smith The ECGs in today’s case are from 3 different patients all presenting with new-onset CP ( ChestPain ). In any case, the ECG is diagnostic of severe ischemia and probably OMI. All ECGs were recorded by EMS, and transferred to a PCI capable center for evaluation.
Written by Pendell Meyers A man in his late 30s with history of hypertension, tobacco use, and obesity presented to the Emergency Department for acute chestpain which started approximately 3 hours prior to arrival, in the setting of a very stressful situation. The pain radiated down both arms, 10/10 in severity.
Written by Jesse McLaren Four patients presented with chestpain. Other signs of OMI that complement the ECG include new regional wall motion abnormalities and refractory ischemia References 1. This will make expert OMI interpretation widely available, and help us continue to learn the subtleties of ECG interpretation 4.
I went to the patient's chart: Elderly woman with stuttering chestpain and SOB, and dizziness. It was normal. == MY Comment , by K EN G RAUER, MD ( 12/26 /2023 ): == It's always rewarding to encounter an ECG that allows you to make an instant clinical pathophysiologic diagnosis. What do you think now?
Another ECG was recorded after the nitroglycerine and now without pain: All findings are resolved. This confirms that the pain was ischemia and is now resovled. The history is concerning ( This patient was awakened from sleep by chestpain that persisted for several hours — on a background of intermittent CP in recent weeks ).
A 60-something yo female presented w/ exertional chestpain for 3 days. Pain was 8/10 and constant. She has been experiencing progressively worsening exertional dyspnea and chest tightness mostly when climbing up flights of stairs since early September. But the patient has active chestpain.
Shortly after receiving epinephrine, the patient developed new leg cramps and chestpain. The chestpain was described as sharp and radiated to both arms. During active chestpain an ECG was recorded: Meyers ECG interpretation: Sinus tachycardia, normal QRS complex, STD in V2-V6, I, II, III and aVF.
Submitted and written by Anonymous, edits by Meyers and Smith A 50s-year-old patient with no known cardiac history presented at 0045 with three hours of unrelenting central chestpain. The pain was heavy, radiated to her jaw with an associated headache. Triage VS: 135/65 mmHg, 95 bpm, 94% on room air, 16/min, 98.6 Abstract 556.
--The STD in V2-V6 might be interpreted as subendocardial ischemia, but with the inferior STE, it is far more likely to represent posterior OMI. Here is the history: A 40-something male had intermittent chest discomfort until 90 minutes prior to presentation, when it became constant. At 100 minutes, the above ECG was recorded.
The patient presented due to chestpain that was typical in nature, retrosternal and radiating to the left arm and neck. He denied any exertional chestpain. It is unclear if the patient was pain free at this time. The ECG does not show any definite signs of ischemia. The below ECG was recorded.
Sent by anonymous, written by Pendell Meyers A man in his 60s presented with acute chestpain with diaphoresis. The ECG was incorrectly interpreted as no signs of ischemia. The Importance of the History: As noted above — the onset of chestpain in today's case was acute. His vitals were within normal limits.
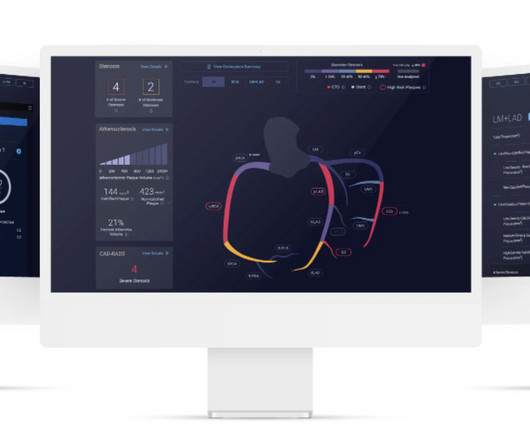
The study describes the validation of Cleerly's artificial intelligence-guided quantitative coronary CT angiography (AI-QCT) ISCHEMIA technology for diagnostic accuracy and prognostic risk stratification. High Diagnostic Accuracy of AI-ISCHEMIA in Comparison to PET, FFR-CT, SPECT, and Invasive FFR: A Pacific Substudy. 2024.01.007.
A 40-something with severe diabetes on dialysis and with known coronary disease presented with acute crushing chestpain. As per Dr. Smith, in a patient with new chestpain — these flattened ST segments in leads V2,V3 suggest acute posterior OMI until proven otherwise. Here is his ED ECG: What do you think?
5 Revascularization to improve blood flow to the heart has been shown to reduce mortality in stable chestpain patients. 6 This novel study marks a significant milestone in the field, evaluating the effectiveness of FFR CT in detecting ischemia-producing coronary stenosis in patients with severe PAD. 10390, May 2023, pp.
Written by Pendell Meyers A woman in her 50s presented with acute chestpain and lightheadedness since the past several hours. The STD maximal in V1-V4 is diagnostic of acute transmural posterior wall ischemia, most likely due to posterior OMI. Subendocardial ischemia does not localize.
The ECG shows severe ischemia, possibly posterior OMI. But cardiac arrest is a period of near zero flow in the coronary arteries and causes SEVERE ischemia. It takes time for that ischemia to resolve. Just as important is pretest probability: did the patient report chestpain prior to collapse?
While in the ED, patient developed acute dyspnea while at rest, initially not associated with chestpain. He later developed mild continuous chestpain, that he describes as the sensation of someone standing on his chest. They agreed ischemia was likely in the setting of demand given DKA and infection.
No prior exertional complaints of chestpain, dizziness, lightheadedness, or undue shortness of breath. He denied headache or neck pain associated with exertion. I sent this ECG to Dr. Smith, with the only information that it is a 17 year old with chestpain. 24 yo woman with chestpain: Is this STEMI?
Written by Jesse McLaren, with edits from Smith A 30 year old with a history of diabetes presented with two days of intermittent chestpain and diaphoresis, which recurred two hours prior to presentation. The chestpain was refractory to nitro so the cath lab was activated: 100% proximal LAD and 99% mid circumflex occlusions.
Submitted and written by Megan Lieb, DO with edits by Bracey, Smith, Meyers, and Grauer A 50-ish year old man with ICD presented to the emergency department with substernal chestpain for 3 hours prior to arrival. At this time he reported ongoing chestpain and was given aspirin and nitroglycerin. J Am Heart Assoc.
These tall T waves are associated with flattening ( straightening ) of the ST segment in the inferior leads — with slight S T elevation in leads V2-thru-V6 ( albeit not enough to qualify as a "STEMI" — Akbar et al, StatPearls, 2023 ). This point is discussed in detail in the March 24, 2023 post of Dr. Smith’s ECG Blog ).
Submitted by Dr. Dennis Cho (@DennisCho), written by Jesse McLaren A 70-year-old with no cardiac history presented with 2 hours of chestpain radiating to the neck, associated with shortness of breath. Acute Q waves are a marker of severe ischemia and a predictor for delayed reperfusion. What do you think?
Submitted by Ali Khan MD and James Mantas MD, MS, written by Pendell Meyers A man in his 50s with history of diabetes, hypertension, and tobacco use presented to the ED with 24 hours of worsening left sided chestpain radiating to the back, characterized as squeezing and pinching, associated with shortness of breath.
Circulation: Cardiovascular Imaging, Volume 16, Issue 11 , Page e015800, November 1, 2023. of patients had evidence of ischemia on a prior functional test. of patients had evidence of ischemia on a prior functional test. were referred to CCTA and 22.5% were referred to CCTA and 22.5% In the follow-up ranging from 1 to 3.5
These were texted to me only with "chestpain." It helps to know that the patient has active chestpain, as Wellen's is a post occlusion (reperfusion) state, with open artery and pain-free. And ECGs can change and evolve even when there is no ischemia. First: 2nd: What was my response? It was indeed.
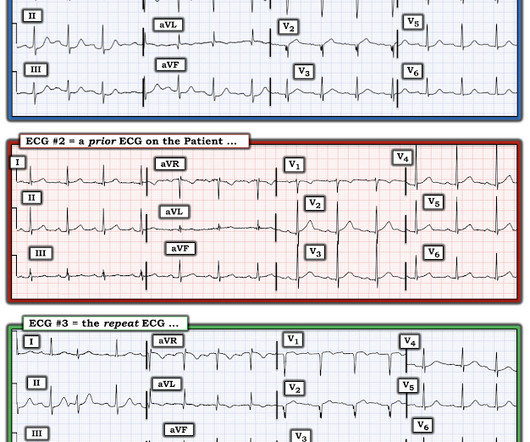
ECG #2 was actually done first, at the time the EMS unit arrived on the scene ( at which time the patient was having severe chestpain ). ECG Blog #184 — illustrates the "magical" mirror-image opposite relationship with acute ischemia between lead III and lead aVL ( featured in Audio Pearl #2 in this blog post ).
Because the patient had no chestpain or shortness of breath, they were initially diagnosed as gastroenteritis. But because the patient had no chestpain or shortness of breath, it was not deemed to be from ACS. But because the patient had no chestpain or shortness of breath, it was not deemed to be from ACS.
Written by Pendell Meyers, with some edits by Smith A man in his 40s with many comorbidities presented to the ED with chestpain, hypotension, dyspnea, and hypoxemia. The flutter waves can conceal or mimic ischemic repolarization findings, but here I don't see any obvious findings of OMI or subendocardial ischemia.
He did not have chestpain. A prior ECG was available for comparison: Normal One might be tempted to interpret the ST depression as ischemia, but as Smith says, "when the QT is impossibly long, think of hypokalemia and a U-wave rather than T-wave." Chestpain in high risk patient. Is it STEMI?
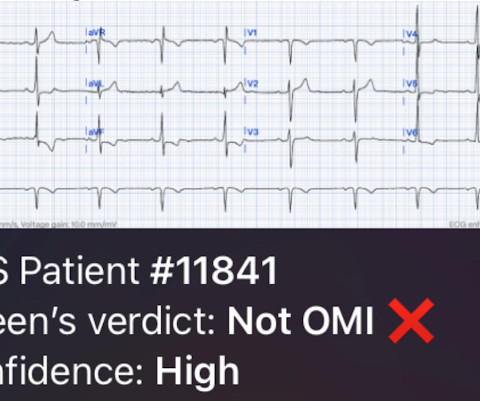
The patient has acute chestpain. Here was my answer: "Not ischemia. This was texted to me in real time. What do you think? Maybe HOCM or another form of LVH. I would not activate cath lab. In this case, QOH was incorrect , saying "OMI High confidence."
Written by Willy Frick A man in his 50s with a history of hypertension, dyslipidemia, type 2 diabetes mellitus, and prior inferior OMI status post DES to his proximal RCA 3 years prior presented to the emergency department at around 3 AM complaining of chestpain onset around 9 PM the evening prior. The following ECG was obtained.
PEARL # 1: Although seeing an elevated Troponin would provide additional support for immediate cardiac catheterization — the clinical reality is that the initial Troponin reading will not always be elevated in patients with acute coronary occlusion ( See March 24, 2023 post in Dr. Smith's ECG Blog ).
Edits by Meyers and Smith A man in his 70s with PMH of hypertension, hyperlipidemia, type 2 diabetes, CVA, dual-chamber Medtronic pacemaker, presented to the ED for evaluation of acute chestpain. EKG shown here: LAFB with no clear signs of OMI or ischemia. Triage ECG: What do you think? This is a huge anterolateral OMI.
Written by Jesse McLaren A 70 year old with prior MIs and stents to LAD and RCA presented to the emergency department with 2 weeks of increasing exertional chestpain radiating to the left arm, associated with nausea. But no ECG met STEMI criteria so the patient was referred to cardiology as Non-STEMI. McLaren and Smith.
On the day of presentation she complained of typical chestpain, and stated it feels like prior MI. ECG#1 Assessing ischemia on an ECG with wide QRS complexes (AIVR, ventricular pacing, BBB, etc) can be challenging. Many health care providers will simply not attempt to assess ischemia in the presence of a wide QRS.
Because previous ischemia induces myocardial preconditioning, decreasing the likelihood of transmural myocardial necrosis and myocardial rupture, patients with evidence of diabetes mellitus, chronic angina or previous MI are less likely to experience a rupture. Not all patients with acute ( or recent ) MI have chestpain with their event.
A 67 yo f developed chestpain this morning." There is probably a trickle of flow which is why there is both subendocardial ischemia (ST depression) and early subepicardial ischemia (hyperacute T-waves). See this case: A man his 50s with chestpain. Figure-1: The initial tracing in today's case. (
He woke up alert and with chestpain which he also had experienced intermittently over the previous few days. The first task when assessing a wide complex QRS for ischemia is to identify the end of the QRS. His wife contacted the ambulance service after the patient experienced an episode of loss of consciousness.
A 60-something awoke with 10/10 crushing chestpain. I would expect TIMI-3 flow (normal flow, no persistent ischemia) with a culprit in the RCA (or possibly Circumflex). But the patient's chestpain continues and so you order a 2nd ECG (ECG 2 here). He walked in to triage.
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chestpain relieved by rest. This episode of chestpain began 3 hours ago and was persistent even at rest. For now she can only say Not OMI.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.















































Let's personalize your content