This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
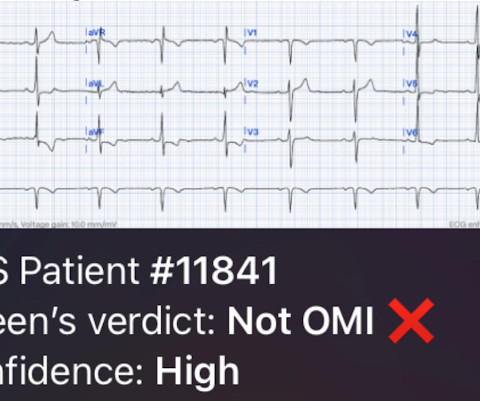
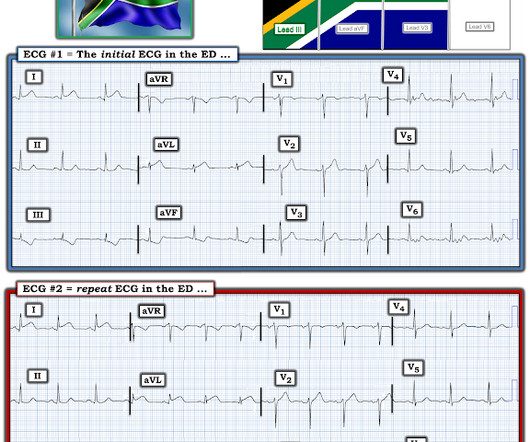
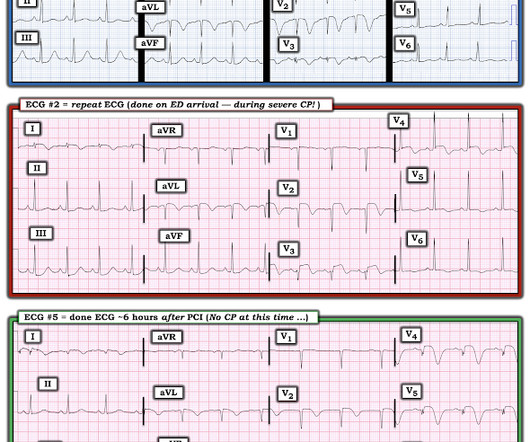
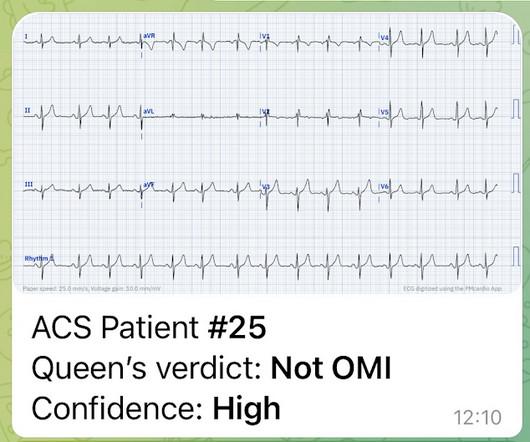
2 middle aged males presented with chestpain. Which had the more severe chestpain at the time of the ECG? Patient 2 at the bottom with a very subtle OMI complained of 10/10 chestpain at the time the ECG was recorded. 414 patients were included in the analysis.
This was sent by anonymous The patient is a 55-year-old male who presented to the emergency department after approximately 3 to 4 days of intermittent central boring chestpain initially responsive to nitroglycerin, but is now more constant and not responsive to nitroglycerin. It is unknown when this pain recurred and became constant.
Of course he said: "Yes, it was a 60 year old diabetic with Chestpain." K en G rauer gives a thorough explanation here: A 60 year old with chestpain == MY Comment , by K EN G RAUER, MD ( 9/15 /2023 ): == The 1st time that I saw APTA ( A rterial P ulse T ap A rtifact ) — I did not know what it was. He said: "What?
I assumed it was a patient with acute chestpain. It was a man in his 30s with chestpain. While statistical likelihood of acute OMI is clearly lower in younger adults — nothing is ruled out by age alone ( as per My Comment in the January 9, 2023 and December 5, 2023 posts in Dr. Smith's ECG Blog ).
For example, considering whatever symptoms that the patient may have had ( ie, chestpain, palpitations, shortness of breath, etc. ) — what this might mean in view of the ECG we are looking at. STEP #2 = Clinical Impression — in which we correlate our assessment that we made in Step #1 to the clinical situation at hand.
A 50-something male had onset of chestpain 1 hour prior to ED arrival. Endorses some associated SOB, but denies back pain, fever, cough, chills, leg swelling, or other new symptoms. Always get serial ECGs in a patient with acute chestpain. It is constant, 9/10, left-sided CP that radiates into left arm and jaw.
Sent by anonymous, written by Pendell Meyers, reviewed by Smith and Grauer A man in his 40s presented to the ED with HTN, DM, and smoking history for evaluation of acute chestpain. He was eating lunch when he had sudden onset chest pressure, 9/10, radiating to his back, with sweating and numbness in both hands.
Written by Pendell Meyers A man in his 60s presented with acute chestpain and normal vital signs. See My Comments at the bottom of the page in the October 6, 2023 and April 17, 2023 posts for review of deWinter T wave patterns ). Here is his triage ECG: What do you think?
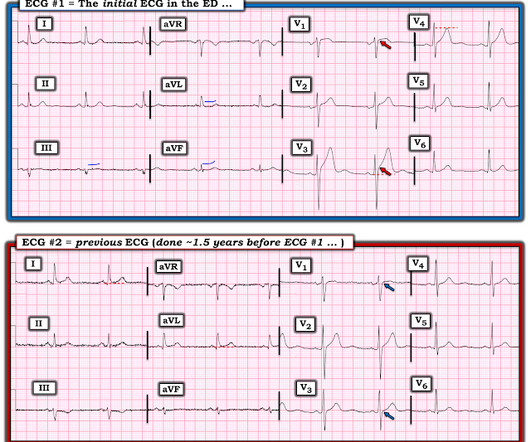
Written by Jesse McLaren A 45 year old presented with two weeks of recurring non-exertional chestpain, now constant for an hour. Because of the ECG changes in a patient with chestpain, and with inferolateral hypokinesis on POCUS, the cath lab was activated. Below is old and then new ECG (old on top; new below).
By Magnus Nossen This ECG is from a young man with no risk factors for CAD, he presented with chestpain. The patient is a young adult male with chestpain. The chestpain was described as pressure like and radiation to both arms and the jaw. How would you assess this ECG? What is your next step?
A 50 year old presented to the emergency department of a remote rural community (where the nearest cath lab is a plane ride away) with one hour of mild chestpain radiating to the back and jaw, and an ECG labeled ‘normal’ by the computer interpretation. What do you think, and how would you manage the patient?
This was sent by Sam Ghali @EM_RESUS A 44 year old man presented with chestpain The tech came running with the ECG as the computer called "STEMI!" What do you think? Sam sent this to me and asked: "What do you think, Steve?" My answer: --Tough one! --But
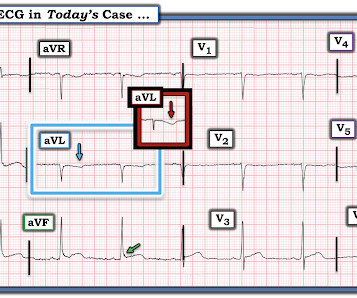
Written by Magnus Nossen with Edits by Grauer and Smith The ECGs in today’s case are from 3 different patients all presenting with new-onset CP ( ChestPain ). We have addresssed this issue on a number of occasions ( See My Comment in the April 25, 2023 — July 21, 2019 — December 10, 2019 — and January 10, 2020 posts).
No ChestPain, but somnolent. The fact that this is syncope makes give it a far lower pretest probability than chestpain, but it was really more than syncope, as the patient actually underwent CPR and had hypotension on arrival of EMS. Here is the ED ECG (a photo of the paper printout) What do you think?
Written by Pendell Meyers A man in his late 30s with history of hypertension, tobacco use, and obesity presented to the Emergency Department for acute chestpain which started approximately 3 hours prior to arrival, in the setting of a very stressful situation. The pain radiated down both arms, 10/10 in severity.
Written by Jesse McLaren Four patients presented with chestpain. All initial ECGs were labeled ‘normal’ or ‘otherwise normal’ by the computer interpretation, and below are the ECGs with the final cardiology interpretation.
I went to the patient's chart: Elderly woman with stuttering chestpain and SOB, and dizziness. It was normal. == MY Comment , by K EN G RAUER, MD ( 12/26 /2023 ): == It's always rewarding to encounter an ECG that allows you to make an instant clinical pathophysiologic diagnosis. What do you think now?
Written by Jesse McLaren, comments by Smith A 55 year old with a history of NSTEMI presented with two hours of exertional chestpain, with normal vitals. See these posts: ChestPain, ST Elevation, and an Elevated Troponin: Should we Activate the Cath Lab? What do you think?
Written by Jesse McLaren A 50 year old presented to triage with one hour of chestpain, and the following ECG labeled normal by the computer (GE Marquette SL) algorithm. As a result "A normal initial Troponin can give false reassurance, when there's a head-on collision happening in real time!" ( from the March 24, 2023 post).
Written by Pendell Meyers A man in his early 40s experienced acute onset chestpain. The chestpain started about 24 hours ago, but there was no detailed information available about whether his pain had come and gone, or what prompted him to be evaluated 24 hours after onset.
Whenever a patient does not have chestpain, the pre-test probability of OMI is diminished. Of course SOB, jaw pain, shoulder pain, etc can be a result of OMI, but the pretest probability is less and so you must scrutinize further. Here is the first ED ECG: COMPUTER INTERPRETATION: Electronic Atrial Pacemaker. the K is 6.8
Written by Jesse McLaren A previously healthy 50 year-old presented with 24 hours of intermittent exertional chestpain, radiating to the arms and associated with shortness of breath. In a previously healthy patient with new and ongoing chestpain, this is concerning for acute occlusion of the first diagonal artery.
A 40-something male presented by ambulance with one hour of chestpain that was improving after sublingual nitroglycerine and 325 mg of aspirin, chewed. Here is his initial ED ECG: What do you think?
A 60-something yo female presented w/ exertional chestpain for 3 days. Pain was 8/10 and constant. She has been experiencing progressively worsening exertional dyspnea and chest tightness mostly when climbing up flights of stairs since early September. But the patient has active chestpain.
Let me tell you about her hospitalization, discharged 1 day prior, but it was at another hospital (I wish I had the ECG from that hospitalization): The patient is 40 years old and presented to another hospital with chestpain and SOB. She had been sitting doing work when she experienced "waves of chest tightness". Sats were 88%.
Sent by anonymous, written by Pendell Meyers A man in his 60s presented with acute chestpain with diaphoresis. Artificial intelligence can be trained to recognize subtle OMI = My Comment by K EN G RAUER, MD ( 2/6 /2023 ): = The initial ECG in today's case was incorrectly interpreted as, "No signs of ischemia".
Case sent by Logan Stark MD, written by Pendell Meyers A woman in her 70s presented with acute chestpain. It started 10 hours prior to arrival, then had improved, then recently returned. No prior ECG was available. Here is her triage ECG: What do you think? The ECG was sent to me with no information, and I replied "OMI".
Written by Jesse McLaren A previously healthy 60 year old developed exertional chestpain with diaphoresis, and called EMS. Here’s the EMS ECG, digitized with PM cardio. What do you think? There’s sinus arrhythmia with normal conduction, normal axis and normal voltages. There’s loss of R waves in V2-3 with hyperacute waves V1-5.
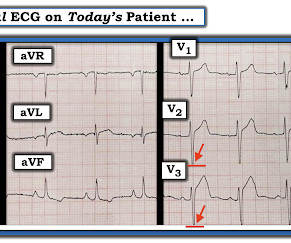
A 40-something with severe diabetes on dialysis and with known coronary disease presented with acute crushing chestpain. As per Dr. Smith, in a patient with new chestpain — these flattened ST segments in leads V2,V3 suggest acute posterior OMI until proven otherwise. Here is his ED ECG: What do you think?
A 40-something woman called 911 in the middle of the night for Chestpain that was intermittent. On arrival, she complained of severe pain. The medics had recorded this ECG and were uncertain whether it was recorded during chestpain: Let's get a better image with use of the PM Cardio app : What do you think?
Submitted by anonymous, written by Pendell Meyers A woman in her 50s presented to the Emergency Department with chestpain and shortness of breath that woke her from sleep, with diaphoresis. See these other cases of arterial pulse tapping artifact: A 60 year old with chestpain Are these Hyperacute T-waves?
There were no injuries and no chestpain and he appeared well. He complained of 3 days of diarrhea and abdominal pain. Pretest probability: Especially when there is no Chestpain, or there are very atypical symptoms, one should be very suspicious of the diagnosis of coronary occlusion unless the ECG is crystal clear.
They had difficulty describing their symptoms, but complained of severe weakness, nausea, vomiting, headache, and chestpain. They described the chestpain as severe, crushing, and non-radiating. Altogether, this strongly suggests inferolateral OMI, particularly in a patient with acute chestpain.
Written by Bobby Nicholson, MD 67 year old male with history of hypertension and hyperlipidemia presented to the Emergency Department via ambulance with midsternal nonradiating chestpain and dyspnea on exertion. Pain improved to 1/10 after EMS administers 324 mg aspirin and the following EKG is obtained at triage.
Submitted and written by Anonymous, edits by Meyers and Smith A 50s-year-old patient with no known cardiac history presented at 0045 with three hours of unrelenting central chestpain. The pain was heavy, radiated to her jaw with an associated headache. Triage VS: 135/65 mmHg, 95 bpm, 94% on room air, 16/min, 98.6
Introduction:The most common acute coronary syndrome (ACS) symptom is chestpain. Chestpain is an umbrella term more precisely described using words like pressure or tightness. Previous studies have not explored the lay public’s conceptions of ACS-related chestpain. were recruited in May and June 2023.
Shortly after receiving epinephrine, the patient developed new leg cramps and chestpain. The chestpain was described as sharp and radiated to both arms. During active chestpain an ECG was recorded: Meyers ECG interpretation: Sinus tachycardia, normal QRS complex, STD in V2-V6, I, II, III and aVF.
Healthy male under 25 years old with a pretty good story for acute onset crushing chestpain relieved with nitro. PEARL: Most patients who present with new chestpain + ECG changes + positive troponin — will not need Cardiac MRI. This was sent to me by a partner: "Curious what you think of this one we had overnight.
My Comment by K EN G RAUER, MD ( 2/22 /2023 ): = Today’s case is an important one, because as per Dr. Smith ( in this patient with new chestpain ) — “The initial ECG is diagnostic of infero-postero OMI.” The presence or absence of ST Elevation is a poor marker with which to describe a myocardial infarction. =
Sent by anonymous, written by Pendell Meyers A man in his 50s with no prior known medical history presented to the Emergency Department with severe intermittent chestpain. He denied any lightheadedness, shortness of breath, vomiting, or abdominal pain. Isn't it amazing?? Don’t Ignore Bedside Echo Results! —
A 50-something presented with acute chestpain. By the way, the patient ruled out for MI by troponins. == MY Comment , by K EN G RAUER, MD ( 6/6/ 2023 ): == Quick cases make for great practice in learning. Here is her ED ECG. It was texted to me while I was out and about. 54-year-old female with CP. And it will only get better.
A 60 year old with chestpain presented to the ED. My Comment by K EN G RAUER, MD ( 1/17 /2023 ): = As per Dr. Smith — pulse - tap artifact used to be a "new" phenomenon to us ( as well as to virtually all medical providers ). Here is his first ECG: What do you think? It looks bizarre, doesn't it? Read more here. =
No prior exertional complaints of chestpain, dizziness, lightheadedness, or undue shortness of breath. He denied headache or neck pain associated with exertion. I sent this ECG to Dr. Smith, with the only information that it is a 17 year old with chestpain. 24 yo woman with chestpain: Is this STEMI?
The patient presented due to chestpain that was typical in nature, retrosternal and radiating to the left arm and neck. He denied any exertional chestpain. It is unclear if the patient was pain free at this time. He has a medical hx notable for hypertension, hyperlipidemia and previous tobacco use disorder.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.







































Let's personalize your content