This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
The VSR is what is causing the cardiogenicshock! Mechanical complications occur acutely and significantly alter hemodynamics leading to comp ensatory mechanism which usually involve vasoconstriction and tachycardia, both hallmarks of cardiogenicshock. PIRP is strongly associated with myocardial rupture.
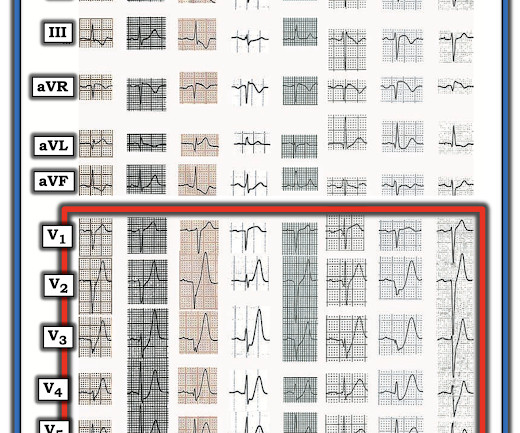
The baseline ECG is basically normal with no ischemia. You can see in the lead-specific analysis that she "sees" the STD in V5, V5, and II, with STE in aVR as signs of "Not OMI", because subendocardial ischemia pattern is not the same as OMI. In my opinion, I think it looks more like subendocardial ischemia.
24 will focus on the following three current guideline updates: American College of Cardiology (ACC)/American Heart Association (AHA) Guidelines 2023 Atrial Fibrillation Guideline - Pharmacology II: Strokes vs. Bleeds, What Do the Guidelines Tell Us About Practical Management in A-fib? The Guidelines Sessions at ACC.24
There is normal R-wave progression in the precordial leads with no evidence of ischemia. Here the image quality is enhanced using the PM Cardio app. What do you think? The presenting ECG shows SR with narrow QRS complexes. In the limb leads there is T-wave inversion in lead aVL with a low amplitude QRS preceding the T-wave.
All of this appears to be consistent with "No Reflow", or small vessel occlusion with persistent ischemia in spite of an open artery. His included cardiogenicshock, V Tach, AV block. --There is persistent ST elevation in leads V1-V4, with a lot of STE in V4 (another bad sign). Such large infarcts have many complications.
The first task when assessing a wide complex QRS for ischemia is to identify the end of the QRS. The ST segment changes are compatible with severe subendocardial ischemia which can be caused by type I MI from ACS or potentially from type II MI (non-obstructive coronary artery disease with supply/demand mismatch). What do you think?
When I was shown this ECG, I said it looks like such widespread ischemia that is might be a left main occlusion, or LM ischemia plus circumflex occlusion (high lateral and posterior OMI). Today's patient did make it to the hospital — but was in cardiogenicshock, and despite valiant attempt at treatment, succumbed soon after.
Remember, in diffuse subendocardial ischemia with widespread ST-depression there may b e ST-E in lead s aVR and V1. There are well formed R-waves with good voltage/amplitude which is uncommon for ischemia. The patient died of cardiogenicshock within 24 hours despite mechanical circulatory support. There are also J-waves.
Session 510) To Treat or Not to Treat Anatomy and Ischemia? Session 508) Battle of the Imagers - Jeopardy Edition! Session 509) Who Wants to Be a Millionaire in Eradicating Vascular Medicine Disparities?
Impella (cardiac output augmentation device) placed for cardiogenicshock Unfortunately, the patient progressed to multiorgan failure with worsening cardiac output despite being maxed on pressors and a balloon pump. EKG shown here: LAFB with no clear signs of OMI or ischemia. He expired 4 days later. No labs were performed.
Whenever there is tachycardia, I am skeptical of OMI unless it has led to severely compromised ejection fracction with cardiogenicshock. The patient was started on heparin for possible NSTEMI vs demand ischemia. increasing stenosis, ischemia, volume changes, increased blood pressure, atrial fibrillation, etc.)
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

















Let's personalize your content