This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Cardiacarrest was called and advanced life support was undertaken for this patient. The patient was given chest compressions while waiting for the cardiacarrest team to arrive. Most such rhythms in the setting of ischemia are VF and will not convert without defibrillation. Calcium level was normal.
The ECG shows severe ischemia, possibly posterior OMI. But cardiacarrest is a period of near zero flow in the coronary arteries and causes SEVERE ischemia. It takes time for that ischemia to resolve. After cardiacarrest, I ALWAYS wait 15 minutes after an ECG like this and record another.
The ECG does not show any definite signs of ischemia. This combination is often extremely effective for maintaining good longterm outcome ( Lanza and Shimokawa — Eur Cardiol 18: e38, 2023 ). The patient presented due to chest pain that was typical in nature, retrosternal and radiating to the left arm and neck.
The H ISTORY in T oday's C ASE: The patient in today's case is a teenager who presented to the ED ( E mergency D epartment ) in cardiacarrest after electrocution. Shark Fin" ST segment elevation is most often a sign of severe transmural ischemia that results from acute coronary occlusion.
Two recent interventions have proven in randomized trials to improve neurologic survival in cardiacarrest: 1) the combination of the ResQPod and the ResQPump (suction device for compression-decompression CPR -- Lancet 2011 ) and 2) Dual Sequential defibrillation. The patient had a volatile clinical course but awoke neuro intact.
We periodically review this intriguing ECG finding that is best known for its association with hypothermia — but which may also be seen in association with a number of other entities, including acute infarction and cardiacarrest. My Comment addresses a few additional aspects of this phenomenon.
See this post: How a pause can cause cardiacarrest 2. It should be kept in mind that on occasions, beta-one agonist can result in increased ventricular ectopy e.g., in severe myocardial ischemia (by increasing myocardial demand), or sometimes with congenital long-QT syndrome. The plan: 1. Place temporary pacemaker 3.
Edited by Bracey, Meyers, Grauer, and Smith A 50-something-year-old female with a history of an unknown personality disorder and alcohol use disorder arrived via EMS following cardiacarrest with return of spontaneous circulation. The described rhythm was an irregular, wide complex rhythm. Circulation. 2001 Nov 27;104(22):2722-7.
PEARL # 1: Although seeing an elevated Troponin would provide additional support for immediate cardiac catheterization — the clinical reality is that the initial Troponin reading will not always be elevated in patients with acute coronary occlusion ( See March 24, 2023 post in Dr. Smith's ECG Blog ).
hours ECG: Not much change hs troponin I peaks at 500 ng/L 8 hours Next morning Urine drug screen: Amphetamine, Methamphetamine, Fentanyl, Fentanyl metabolite Formal Bubble Contrast Echocardiogram: Indications for Study: Silent Ischemia. Conclusion: Type II MI probable due to hypoxia and tachycardia from resp arrest and amphetamine use.
They had had twice the rate of cardiacarrest and twice the in-hospital mortality[1] In another study of patients diagnosed with STEMI, those on dialysis experienced delayed reperfusion and double the mortality.[2] They were less likely to have STEMI on ECG, and more likely to be initially diagnosed as non-ACS.
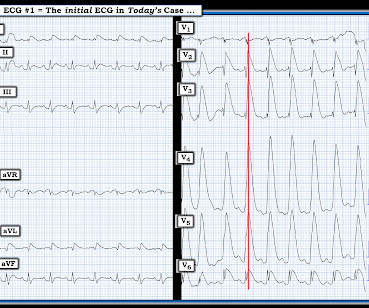
= Case Presentation by K EN G RAUER, MD ( 5/5 /2023 ): — Edits by Drs. Meyers & Smith. = Dr. Smith was reading ECGs — and he sent myself and Dr. Meyers the tracing shown in Figure-1. At the time we did not yet know the history. What do YOU think? Figure-1: The initial ECG in today's case. No history yet.
This suggests ischemia of uncertain duration. Unfortunately, before this could be accomplished — the patient went into cardiacarrest. She was successfully resuscitated — with a post-arrest rhythm similar to that seen in Figure-1. Cardiac cath did not reveal significant coronary disease!
What is the cardiac rhythm shown in the long lead II rhythm strip? Figure-1: The initial ECG in today’s case — obtained from an elderly woman following successful resuscitation from cardiacarrest. ( To improve visualization — I've digitized the original ECG using PMcardio ). What about the 1 2- L ead E CG ?
The first task when assessing a wide complex QRS for ischemia is to identify the end of the QRS. The ST segment changes are compatible with severe subendocardial ischemia which can be caused by type I MI from ACS or potentially from type II MI (non-obstructive coronary artery disease with supply/demand mismatch). What do you think?
A prior ECG was available for comparison: Normal One might be tempted to interpret the ST depression as ischemia, but as Smith says, "when the QT is impossibly long, think of hypokalemia and a U-wave rather than T-wave." Polymorphic Ventricular Tachycardia Long QT Syndrome with Continuously Recurrent Polymorphic VT: Management CardiacArrest.
Remember, in diffuse subendocardial ischemia with widespread ST-depression there may b e ST-E in lead s aVR and V1. There are well formed R-waves with good voltage/amplitude which is uncommon for ischemia. Smith: This bizarre ECG looks like a post cardiacarrest ECG with probable acidosis or hyperkalemia in addition to OMI.
When I was shown this ECG, I said it looks like such widespread ischemia that is might be a left main occlusion, or LM ischemia plus circumflex occlusion (high lateral and posterior OMI). Suffice it to say that, "The heart does whatever it will do when a patient is about to arrest". There is STE in aVR.
Food and Drug Administration (FDA) approved the first anti-inflammatory therapeutic option to reduce cardiac event risk in patients with established cardiac risk factors. As of June 2023, the U.S. Accessed November 8, 2023. Accessed January 18, 2023. AGEPHA Pharma FZ LLC; 2023. 12 Colchicine, 0.5
Brugada Syndrome: Diagnosis and Risk Stratification Hello friends, this is the modified version of my talk at Indian Heart Rhythm Society Conference, New Delhi, 2023, on Brugada Syndrome. Hope you will enjoy this session. These are the conditions which have to be considered or excluded as they can sometimes manifest Brugada pattern on ECG.
2017 AHA/ACC/HRS guideline for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death. Heart Rhythm, 15(9): 1394-1401. [7] 7] American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society.
The patient was unconscious BEFORE the cardiacarrest, at the same time that she had strong pulses. Therefore, cardiacarrest is NOT the etiology of the coma. More cases here to highlight: [link] Middle Aged Woman with Asystolic CardiacArrest, Resuscitated: Cath Lab? OMI is a clinical diagnosis.
Unexplained cardiacarrest or documented VF/polymorphic VT: +3 3. Unexplained sudden cardiac death (3 categories) (+0.5 - +2) 4. Among potential conditions that may produce Brugada Phenocopy are infarction and ischemia. Ischemia or infarction. Cardiacarrest. Clinical History 2.a. Family History 3.a.
Occurrence of “J Waves” in 12-Lead ECG as a Marker of Acute Ischemia and Their Cellular Basis. Occurrence of "J waves" in 12-lead ECG as a marker of acute ischemia and their cellular basis. 2004 = My Comment by K EN G RAUER, MD ( 1/21 /2023 ): = I thought today's case by Drs. Pacing Clin Electrophysiol.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






























Let's personalize your content