This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
The chestpain quickly subsided. Cardiacarrest was called and advanced life support was undertaken for this patient. The patient was given chest compressions while waiting for the cardiacarrest team to arrive. After about 90 seconds of chest compressions she awoke. Calcium level was normal.
But cardiacarrest is a period of near zero flow in the coronary arteries and causes SEVERE ischemia. After cardiacarrest, I ALWAYS wait 15 minutes after an ECG like this and record another. Just as important is pretest probability: did the patient report chestpain prior to collapse?
Let me tell you about her hospitalization, discharged 1 day prior, but it was at another hospital (I wish I had the ECG from that hospitalization): The patient is 40 years old and presented to another hospital with chestpain and SOB. She had been sitting doing work when she experienced "waves of chest tightness". Sats were 88%.
The patient presented due to chestpain that was typical in nature, retrosternal and radiating to the left arm and neck. He denied any exertional chestpain. It is unclear if the patient was pain free at this time. He has a medical hx notable for hypertension, hyperlipidemia and previous tobacco use disorder.
Two recent interventions have proven in randomized trials to improve neurologic survival in cardiacarrest: 1) the combination of the ResQPod and the ResQPump (suction device for compression-decompression CPR -- Lancet 2011 ) and 2) Dual Sequential defibrillation. The patient had a volatile clinical course but awoke neuro intact.
Because the patient had no chestpain or shortness of breath, they were initially diagnosed as gastroenteritis. But because the patient had no chestpain or shortness of breath, it was not deemed to be from ACS. Potassium was normal. Cardiology did not think it was "STEMI", but repeated the troponin. Take home 1.
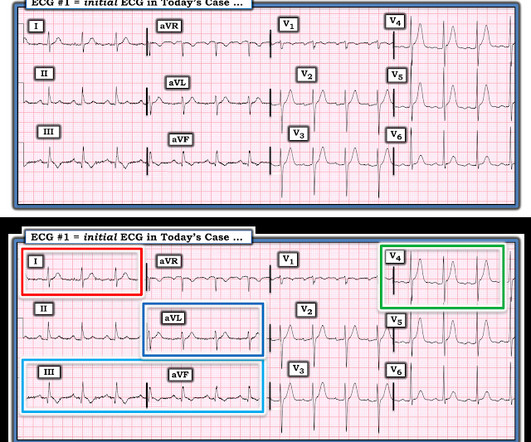
Shortly after arrival in the ED ( E mergency D epartment ) — she suffered a cardiacarrest. BUT — Cardiac catheterization done a little later did not reveal any significant stenosis. Figure-1: The initial ECG in today's case — obtained after successful resuscitation from cardiacarrest. ( No CP ( C hest P ain ).
The ECG in Figure-1 — was obtained from a middle-aged man who presented to the ED ( E mergency D epartment ) in cardiacarrest. C ASE C onclusion: As noted above — the middle-aged man in today's case presented to the ED in cardiacarrest. In view of this history — How would YOU interpret the ECG in Figure-1 ?
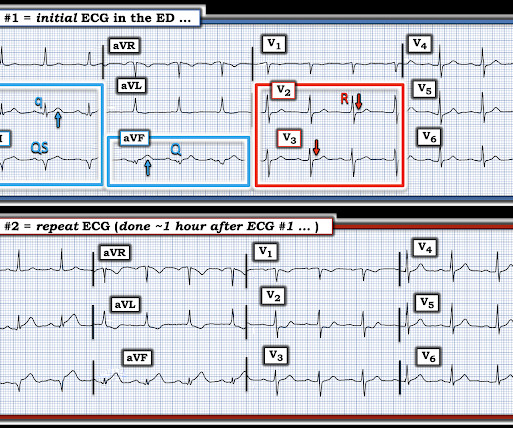
PEARL # 1: Although seeing an elevated Troponin would provide additional support for immediate cardiac catheterization — the clinical reality is that the initial Troponin reading will not always be elevated in patients with acute coronary occlusion ( See March 24, 2023 post in Dr. Smith's ECG Blog ). BLUE arrows in Figure-2 ).
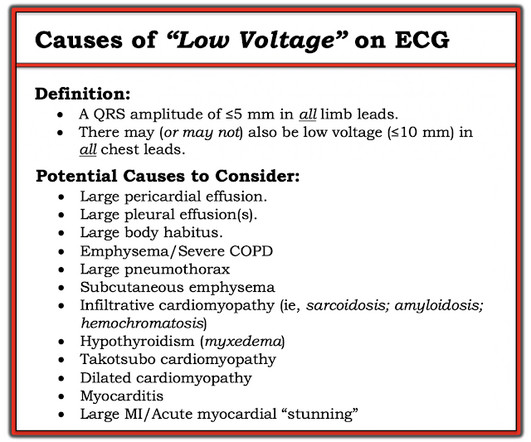
This middle aged patient presented with chestpain: What do you think? link] == MY Comment , by K EN G RAUER, MD ( 12/11 /2023 ): == As per Dr. Smith — the KEY concept in today's case is proportionality. There is VERY low voltage. There is some ST Elevation, but it is MINIMAL. But look how small the QRS is!!
And she does not know that this is an overdose; she thinks it is a patient with chestpain!! Severely ill patients from any etiology can have very abnormal ECGs = My Comment by K EN G RAUER, MD ( 5/26 /2023 ): = There are more questions than answers in today's case. 3 hours later, this was recorded at a K of 2.8
Given the history of dyspnea on exertion over a several week period ( but no mention of chestpain ) — and — the finding of deep, symmetric T wave inversion in the anterior leads ( as per Pearl #2 ) — it is possible that the onset of her symptoms is the result of a "Silent MI" ( See ECG Blog #228 for more on "Silent" MI ). . =
He did not have chestpain. Polymorphic Ventricular Tachycardia Long QT Syndrome with Continuously Recurrent Polymorphic VT: Management CardiacArrest. Chestpain in high risk patient. Here is his triage ECG: What do you think? What does the ECG show? Also see the bizarre Bigeminy. Is it STEMI?
He woke up alert and with chestpain which he also had experienced intermittently over the previous few days. The history in today's case with sudden loss of consciousness followed by chestpain is very suggestive of ACS and type I ischemia as the cause of the ECG changes. What do you think?
Some patients have baseline RBBB with LAFB, but in patients with likely ACS, these are associated with severe infarction with cardiacarrest, cardiogenic shock or impending shock. Here are some cases of RBBB with LAFB: What is the Diagnosis in this 70-something with ChestPain?
All of the patients presented with chestpain , and they are all in triage. Smith: This bizarre ECG looks like a post cardiacarrest ECG with probable acidosis or hyperkalemia in addition to OMI. Which, if any, of these patients has OMI, with myocardium at risk and need for emergent PCI? What was the pH and K?
Written by Pendell Meyers A man in his 70s with no cardiac history presented with acute weakness, syncope, and fever. He denied chestpain or shortness of breath. In the clinical context of weakness and fever, without chestpain or shortness of breath, the likelihood of Brugada pattern is obviously much higher.
This patient had many complaints including chestpain. Comment by K EN G RAUER, MD ( 2/11 /2023 ): = Today’s case is from a patient with “many complaints”, including chestpain — and, an ECG that raised concern about acute anterior OMI. Chestpain was just one of these complaints. mEq/L (very high).
Here is the history: 62 yo male w 2d of intermittent chestpain, now constant. Here is a more detailed history: Presented to the emergency department with chestpain. Patient states that he began to develop substernal chestpain two days ago. ng/ml) The sender asked: "Would you activate the cath lab?"
Written by Pendell Meyers, sent by anonymous, with additions by Smith A man in his 40s had acute chestpain and called EMS. 3) [link] Artificial intellingence based detection of acute coronary occlusion compared to STEMI criteria - External validation study in a consecutive all-comer German chestpain unit cohort.
A middle-age woman with no previous cardiac history called 911 for chestpain. A retrospective 'target trial emulation' comparing amiodarone and lidocaine for adult out-of-hospital cardiacarrest resuscitation. This was her prehospital ECG: What do you think? DOI: 10.1016/j.resuscitation.2025.110515
A 50-something male presented to triage with chestpain for one day. A Chest X-ray showed infiltrates. Thus, another etiology of chestpain is found, and the fever suggests "fever-induced Brugada." Unexplained cardiacarrest or documented VF/polymorphic VT: +3 3. Cardiacarrest.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


























Let's personalize your content