This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
ABSTRACT Background Despite leadless pacemakers (LPMs) showing promise, real-world data comparing them to transvenous pacemakers (TV-VVI) are insufficient and often contradictory, especially in patients without major comorbidities like heart failure. Objectives Comparing LPMs with TV-VVIs in real-world patients without HF.
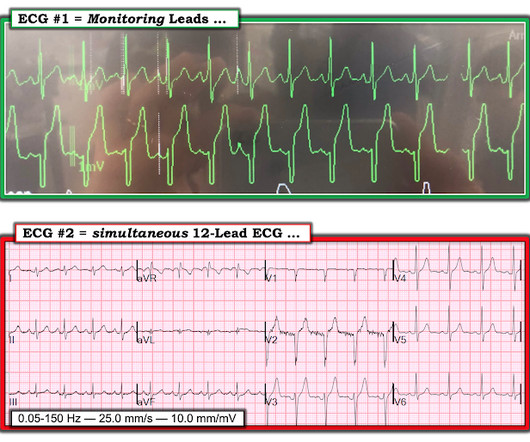
= Case Presentation by K EN G RAUER, MD ( 5/5 /2023 ): — Edits by Drs. The "good" news — Treatment with naloxone will probably resolve the bradycardia. Meyers & Smith. = Dr. Smith was reading ECGs — and he sent myself and Dr. Meyers the tracing shown in Figure-1. At the time we did not yet know the history. What do YOU think?
Discontinue all negative chronotropic agents, since the risk of torsade is much higher with bradycardia or pauses. Place temporary pacemaker 3. For more on Torsades de Pointes vs PMVT See My Comment in the October 18, 2023 post and the September 2, 2024 post in Dr. Smith's ECG Blog ). The plan: 1.
Written by Willy Frick A man in his 70s with a history of HFrEF and sick sinus syndrome s/p dual chamber pacemaker placement was admitted for overnight observation following outpatient placement of a mitral valve clip. This is unambiguous evidence of pacemaker malfunction. Imagine the pacemaker is set at a minimum rate of 60.
LP, leadless pacemaker; PCT, pacing capture threshold; AUC, area under the curve. ABSTRACT Introduction Leadless pacemakers (LPs) are a valuable treatment for bradycardia, with the Aveir offering advanced features, including a protective sleeve and active fixation. A PCT elevation was defined as that >1.5V/0.4ms
Is a pacemaker needed? Even if we stopped here — We could conclude the following: There is marked bradycardia in today's rhythm ( ie, Heart rate in the low 30s ). Finally — If today's patient does not have significant underlying coronary disease — then her bradycardia with AV block may be the result of SSS ( S ick S inus S yndrome ).
to 1828 msec. ) — which corresponds to a variation in the rate of sinus bradycardia from 36-to-33/minute. This makes sense given that the underlying rhythm in today's case appears to be marked sinus bradycardia and arrhythmia , with a ventricular escape rhythm appearing when the SA node rate drops below 33/minute.
That said — obvious findings include: i ) Marked bradycardia! — My Immediate Impression — was that this elderly woman with a several week history of symptoms would most likely leave the hospital with a pacemaker. The rhythm in Figure-1 is complex — and defies precise interpretation without careful study. be regular! —
link] == MY Comment , by K EN G RAUER, MD ( 11/11 /2023 ): == From a learning standpoint — I LOVED this case because it illustrates in many ways how some patients simply "do not read the textbook before they come to the ED". It is not yet available, but this is your way to get on the list.
In fact, sometimes the sinus node is working and acting as a pacemaker but no P waves are visible!! These T-waves are tall but have a narrow base and a corresponding flat ST segment (see lead V4). Also, there are no definite P-waves and this is another result of hyperkalemia. This is called sino-ventricular rhythm. The patient was treated.
After the heart rate increased slightly, here was the repeat ECG: Sinus bradycardia, only slightly faster rate than prior. Hint: there are 2 etiologies) = Comment by K EN G RAUER, MD ( 2/23 /2023 ): = As today's case was contributed by Dr. Nossen, who practices in Norway — today's ECG uses the Cabrera Format.
milla1cf Fri, 01/19/2024 - 10:55 January 19, 2024 — Orchestra BioMed , a biomedical company accelerating high-impact technologies to patients through risk-reward sharing partnerships, today announced the first patient was randomized in the BACKBEAT pivotal study in late December 2023. Orchestra BioMed and Medtronic, Inc. Kowal, M.D.,
My Comment by K EN G RAUER, MD ( 3/15 /2023 ): = I found today’s case highly instructive in highlighting a number of important aspects regarding the presentation and initial treatment of a patient who presents to the ED with new AFib. Baseline bradycardia in endurance athletes limits the use of ß-blockers.
Isoprenalin was discontinued, and a temporary transveous pacemaker was implanted. The patient stabilized following pacemaker placement. For example — bradycardia and AV conduction disturbances are not uncommon with Hyperkalemia , with these conduction disturbances most often resolving once serum K+ is corrected.
To improve visualization — I've digitized the original ECG using PMcardio ) MY Thoughts on the ECG in Figure-1: This is a challenging tracing to interpret — because there is marked bradycardia with an irregular rhythm and a change in QRS morphology. Figure-1: The initial ECG in today's case. ( The QRS complex is wide ( ie, >0.10
Within ten minutes, she developed bradycardia, hypotension, and ST changes on monitor. Bradycardia and heart block are very common in RCA OMI. 2:34 PM, following right heart catheterization She then went into atrial fibrillation with complete heart block and junctional escape rhythm prompting placement of transvenous pacemaker.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






















Let's personalize your content