This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
There is a regular narrow complex tachycardia. Thus, it is supraventricular tachycardia. It is important to remember that SVT includes Sinus Tachycardia! Sometimes even Wide Complex Tachycardia is Sinus. See this case in which Lewis leads were necessary to figure this out: Wide Complex Tachycardia.
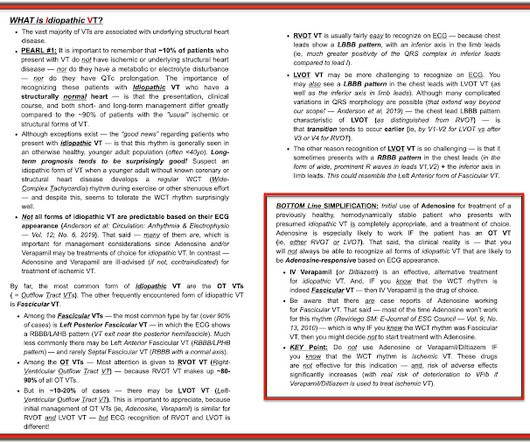
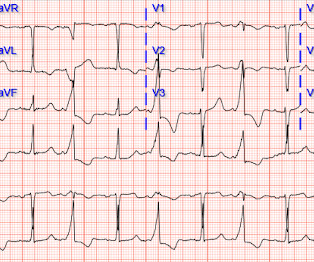
A prehospital 12-lead was recorded: There is a regular wide complex tachycardia. The computer diagnosed this as Ventricular Tachycardia. There is a wide complex regular tachycardia at a rate of 226. Toothache, incidental Wide Complex Tachycardia Could it be fascicular VT or Bundle Branch VT ( i.e., idiopathic VT )?
She had a single chamber ICD/Pacemaker implanted several years prior due to ventricular tachycardia. Answer : The ECG above shows a regular wide complex tachycardia. Said differently, the ECG shows a rather slow ventricular tachycardia with a 2:1 VA conduction. Cardiac output (CO) was being maintained by the tachycardia.
A patient in the ICU with significant underlying cardiac disease [HFrEF 30%, non-ischemic cardiomyopathy, LBBB s/p CRT-D (biventricular pacer), AVNRT s/p ablation a few yrs ago, hx sinus tachycardia while on max tolerated BB therapy] went into a regular wide-complex tachycardia after intubation for severe COPD exacerbation. What to do?
We would like to comment on the publication “Postural orthostatic tachycardia syndrome after COVID-19 vaccination [1].” This study evaluated patients who received the mRNA COVID-19 vaccine and then developed new or worsening symptoms of Postural Orthostatic Tachycardia Syndrome (POTS).
An Initial ECG was performed: Initial ECG: Sinus tachycardia with prolonged QT interval (QTc of 534 ms by Bazett). She was admitted to the ICU where subsequent ECGs were performed: ECG at 12 hours QTc prolongation, resolution of T wave alternans ECG at 24 hours Sinus tachycardia with normalized QTc interval. 2022 Jul;27(4):e12939.
The ECG shows sinus tachycardia with RBBB and LAFB, without clear additional superimposed signs of ischemia. Retrieved July 2, 2022, from [link] Moyé, D. Retrieved July 2, 2022, from [link] Sybrandy, K. He was intubated for altered mental status. Chest trauma was suspected on initial exam. References Alborzi, Z., Zangouri, V.,
It's a very "fun" ECG, with initial ectopic atrial tachycardia (negative P waves in inferior leads conducting 1:1 with the QRSs), followed by spontaneous resolution to sinus rhythm. What About the Tachycardia? Today's regular SVT rhythm could be an ectopic atrial tachycardia ( ATach ) — or an automatic junctional tachycardia.
It shows sinus tachycardia with right bundle branch block. Taking a step back , remember that sinus tachycardia is less commonly seen in OMI (except in cases of impending cardiogenic shock). As per Dr. Frick — sinus tachycardia is usually not seen with acute OMI unless the patient is in cardiogenic shock. Both were wrong.
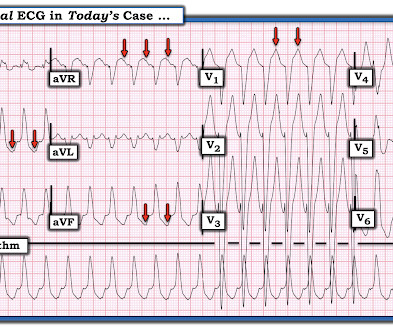
Because of this, it is uncommon to see sinus tachycardia with a prolonged PR interval. And I wish I had record of ECG monitoring just before — and during — and just after the rhythm changes from the regular tachycardia in ECG #1 — to the bigeminal rhythm in ECG #2. This is precisely what we see in Figure-6.
Sinus tachycardia has many potential causes. This is especially true for the elderly patient with sinus tachycardia. What is the cause of the sudden tachycardia? She had a very elevated troponin T at 12,335 ng/L at the time of presentation. The patient in today’s case suddenly became tachycardic while sleeping.
Abstract Introduction The utility of ablation index (AI) to guide ventricular tachycardia (VT) ablation in patients with structural heart disease is unknown. Methods Consecutive patients ( n = 103) undergoing initial VT ablation at a single center from 2017 to 2022 were evaluated.
This strip was obtained: Apparent Wide Complex Tachycardia at a rate of 280 What do you think? Troponins 34>33>43, likely secondary to myocardial injury from tachycardia. Sinus tachycardia does not go this fast. A 60-something ow healthy male had syncope while on treadmill. What do you want to do?
Sacubitril/valsartan can improve outcomes for patients with heart failure and ventricular tachycardia, but few studies examined whether it can reduce recurrence or improve cardiovascular outcomes in patients with persistent atrial fibrillation after catheter ablation.
This is sinus tachycardia (rhythm) with complete heart block (AV node function) with ventricular escape rate just below 30. Never forget that sinus tachycardia is the scariest arrhythmia. The April 17, 2022 post ( Leads V1,V2 misplacement ). The May 5, 2022 post ( LA-RA reversal ).
You are shown the ECG in Figure-1 — told only that the patient had a “continuous" tachycardia. PEARL # 4: This less common form of "fast-slow" AVNRT that is illustrated in Figure-3 — has also been known as an "incessant" tachycardia. ECG Blog #138 — AFlutter vs Atrial Tachycardia. What is the differential diagnosis?
The primary endpoint was any AF or atrial tachycardia recurrence at 12 and 24 month follow up.Resultsthe study cohort was composed by 138 patients (mean age was 5911 years, 38% female) and successful PVI was achieved in 100% of cases. Procedural data and electrophysiology (EP) laboratory times were systematically collected and analyzed.
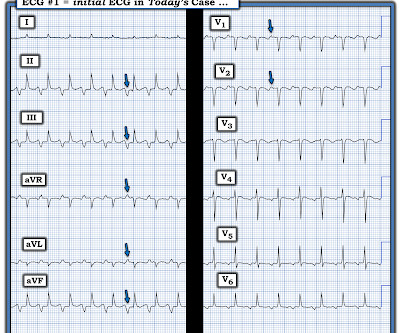
EMS reports intermittent sinus tachycardia and bradycardia secondary to some type of heart block during transport. It is hard to make out P waves but you can see them best in V2, and notches in the T waves in other leads - this is a sinus tachycardia with a very long PR interval indicating first degree block.
Artifact can obscure the rhythm or cause misdiagnosis of rhythms such as atrial fibrillation, ventricular tachycardia, and ventricular fibrillation. Instead — lead III tells us that the underlying rhythm is sinus tachycardia at 100-105/minute.
This point is particularly relevant regarding ECG #2 — because sinus tachycardia is seen on this earlier ECG. In the October 15, 2022 post of Dr. Smith's ECG Blog — Drs. Smith and Meyers in their October 15, 2022 post on Precordial Swirl. What is P recordial S wirl ? NOTE: It's EASY to get fooled by LVH!
Here is his ED ECG: Regular Wide Complex Tachycardia at a rate of 229 First : What do you want to do? Before getting into analysis, a regular wide complex tachycardia could be 1. ventricular tachycardia ( VT ) or 2. AV reciprocating tachycardia ( AVRT , antidromic WPW) or 3. Next : What do you think is the ECG diagnosis?
Tachycardia and ST Elevation. == MY Comment , by K EN G RAUER, MD ( 7/7 /2024 ): == Among the most rewarding type of case for me during my days working in the ED — would be seeing a patient who presented with acute CP ( C hest P ain ) — who I would be able to “cure” simply by recognizing and treating their arrhythmia. Would you give lytics?
I focus my thoughts on a qualitative approach to these 3 pre-hospital ECGs — all obtained from patients presenting with acute CP ( C hest P ain ). == ECG #1 — from a 70-ish year old Woman with acute CP and Dyspnea The rhythm is sinus tachycardia at a surprisingly rapid rate of ~115/minute. African Flag Sign that is not quite fulfilled here ).
I’ve previously reviewed specific ECG findings to look for ( See My Comment at the bottom of the page in the September 1, 2020 post — the March 4, 2023 post — and, in the March 6, 2022 post , among others. KEY Findings in ECG #1 include the following: Sinus tachycardia at ~110/minute. Junctional tachycardia? ).
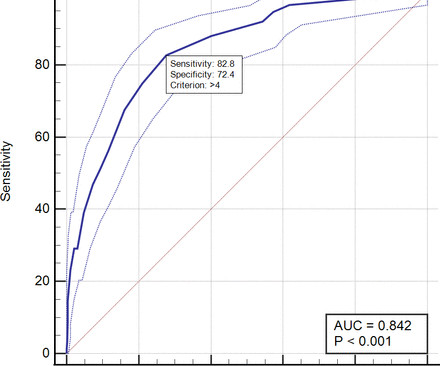
Methods This retrospective cohort study included all ACS patients aged≥18 years who were admitted to Dr. Hasan Sadikin Central General Hospital from January 2018 to January 2022. The area under the curve (AUC) among PADMA, GRACE, C-ACS and ProACS risk scores was compared using the fisher Z test.
We see a regular tachycardia with a narrow QRS complex and no evidence of OMI or subendocardial ischemia. The differential of a regular narrow QRS tachycardia is sinus tachycardia, SVT, and atrial flutter with regular conduction. Now the patient is in sinus tachycardia. Her initial EKG is below. Same as initial ECG.
This one is far more specific, as it is combined with sinus tachycardia and some T-wave inversion in V1-V3. and tachycardia, 1.8. Finally , they found that S1Q3T3, precordial T-wave inversions V1-V4, and tachycardia were independent predictors of PE. This is a classic S1Q3T3. Most S1Q3T3 is not due to PE. incomplete RBBB 1.7
This usually represents posterior OMI, but in tachycardia and especially after cardiac arrest, this could simply be demand ischemia, residual subendocardial ischemia due to the low flow state of the cardiac arrest. The April 8, 2022 post by Drs. This prompted cath lab activation. There is profound ST depression maximal in V1-V4.
Abstract Introduction The use of flecainide and propafenone for medical cardioversion of atrial fibrillation (AF) and atrial flutter/intra-atrial reentrant tachycardia (IART) is well-described in adults without congenital heart disease (CHD). The unit of analysis was each episode of AF/IART.
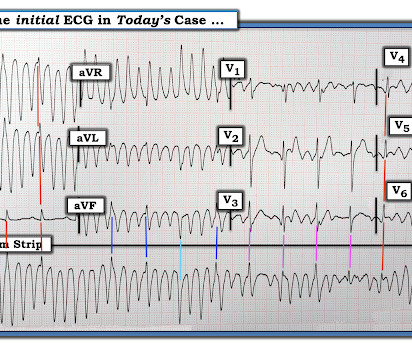
From afar, there is gross tachycardia, cadence irregularities, and narrow QRS complexes that may, or may not, be Sinus in origin; and finally – a cacophony of wide complexes that might very well be ventricular in origin. McLaren : We’ve answered the first question – Sinus Tachycardia with episodic runs of wide QRS (RBBB morphology) and PVC’s.
Descriptive analysis of the ECG in today's case reveals a regular, narrow tachycardia at ~130/minute , without clear sign of sinus P waves. But the rate is ~130/minute — which is a bit fast for sinus tachycardia. So IF this is sinus tachycardia with a sinoventricular rhythm — then we have to explain WHY the rate is this fast.
The ECG there reportedly showed an irregular tachycardia, and the patient was immediately referred to the emergency room. Here is her ECG on arrival: There is a wide complex tachycardia that is irregularly irregular (this is difficult to determine at these very high rates). Vitals were within normal limits other than heart rate.
Although ECG signs of acute PE typically involve inferior and/or anterior lead ST depression/T wave inversion — on occasion, there can be ST elevation ( Gheith et al — Cureus 14(9): e29249, 2022 — and — Siddiqa et al — Am J Case Reports 21: e927923-6, 2020 ). There is sinus tachycardia at ~100/minute. As per Dr.
Another way that WPW can be concealed is in the very rare (~15% of all WPW patients) retrograde-only conduction, in which the accessory pathway ONLY allows retrograde conduction, which obviously wouldn't show a delta wave on sinus EKG but still predisposes the patient to re-entry tachycardias. And why is the PR interval not short? Khouzam RN.
It should be treated as such unless there is more information such as old or serial EKGs that can confirm a benign diagnosis, as BTWI patterns can mimic the South Africa Flag Sign (Compare this EKG to case 4 here: [link] com/2022/05/quiz-post-which- of-these-if-any-are-omi.html ). Patient 1 remained in the hospital overnight. It was stented.
ACUTE MI (I allowed Acute MI to be in the report because I knew there would be an elevated troponin from ischemia, which is the definition of acute MI -- but in this case it would most likely be a Type 2 MI from tachycardia) There is also LA-RA lead reversal. The April 17, 2022 post ( Leads V1,V2 misplacement ).
22:25 — What if you have a regular SVT ( = narrow-complex tachycardia ) without obvious P waves? ( 25:00 — The advantage of getting a 12-lead in an unknown tachycardia = “12 Leads are Better than One” ( = You have 12 leads to tell if the QRS is wide or narrow! ). ). 19:50 — Not appreciating statistical odds! ( The 4 common causes? —
Routine STEMI activation in STE-aVR for emergent revascularization is not warranted, although urgent, rather than emergent, catheterization appears to be important. == MY Comment, by K EN G RAUER, MD ( 11/4 /2022 ): == Our thanks to Drs. A slightly prolonged QTc ( although this is difficult to assess given the tachycardia ).
Blunt Trauma in a Child 40-something male in a head-on Motor Vehicle Collision and Splenic Injury == MY Comment, by K EN G RAUER, MD ( 10/10 /2022 ): == Highly interesting post by Dr. Smith regarding a 30-something male with multiple injuries from a motor vehicle accident. Sinus Tachycardia ( common in any trauma patient. ).
T-wave inversions and dynamic ST elevation Tachycardia, hyperthyroid, and ST elevation. Please see My Comment at the bottom of the page in the April 17, 2022 post of Dr. Smith's Blog — for concise review on how to quickly recognize too-high placement of the lead V1 and V2 electrodes. What is it? Anterior STEMI? Activate the Cath Lab?
The ECG shows sinus tachycardia, a narrow, low voltage QRS with alternating amplitudes, no peaked T waves, no QT prolongation, and some minimal ST elevation in II, III, and aVF (without significant reciprocal STD or T wave inversion in aVL). It is difficult to tell if there is collapse during diastole due to the patient’s tachycardia.
In addition to sinus tachycardia, the only abnormalities listed by the computer were "low voltage, precordial leads" and "anteroseptal infarct, old.Q This is something that is hard to teach, but with hundreds of such cases, we have taught the artificial intelligence algorithm to recognize this. 4) There is well formed J-point notching.
There is sinus tachycardia at 100-105/minute. The scooped shape of this ST depression in lead V2 makes for a positive " Mirror " Test ( For my thoughts on the Mirror Test — See My Comment in the September 21, 2022 post in Dr. Smith's ECG Blog ). Figure-1: Comparison of the first 3 ECGs in today's case. Axis and intervals are normal.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.











































Let's personalize your content