This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Stent performance was assessed.ResultsWe identified 28 patients (67.8% The procedures mostly used 7 Fr sheaths for stents on 6, 7, and 8 mm balloons and 8 Fr sheaths for 9, 10, 12 mm balloons. Median stent expansion percentage was 95% (IQR, 90%96%). Median stent shortening was 1.9% (IQR, 0%3.9%). kg (IQR, 9.116.4).
M2‐M4, ACA, and PCA) who underwent thrombectomy over 5 years (2018‐2022) at a single comprehensive stroke center. M2‐M4, ACA, and PCA) who underwent thrombectomy over 5 years (2018‐2022) at a single comprehensive stroke center. Primary safety outcome is rate of complications associated with the stent retriever.
BACKGROUND:In patients with post-thrombotic syndrome, stent recanalization of iliofemoral veins or the inferior vena cava can restore venous patency and improve functional outcomes. The risk of stent thrombosis is particularly increased during the first 6 months after intervention.
A bare metal stent (BMS) may protect LGO, according to the hypothesis of this single-center retrospective analysis.MethodsAll patients undergoing elective EVAR with a bifurcated stent graft between January 2012 and June 2022 were included in this cohort study.
Former resident: "Just saw cath report, LAD stent was 100% acutely occluded." They of course opened and stented it. They said it looked similar to his old one (in my opinion, similar, but not similar enough to be able to say no OMI)." Smith : "What was the outcome?" You taught us well!"
Webinar New FDA-Approved Aortic Technologies kchalko Thu, 11/10/2022 - 12:30 November 3, 2022 Recent approvals by the U.S. The Thoraflex Hybrid Frozen Elephant Trunk (FET) device is a pre-mated surgical graft and an aortic stent graft to facilitate single-stage treatment of arch and proximal descending aortic pathologies.
I advised that perhaps posterior leads would help to persuade the interventionalist, since the 2022 ACC recommendations include posterior STEMI as a formal STEMI equivalent, but only officially by 0.5 Angiogram reportedly showed acute thrombotic occlusion of the first obtuse marginal which was stented. mm STE in the posterior leads.
BACKGROUNDThe optimal reperfusion technique in patients with isolated posterior cerebral artery (PCA) occlusion is uncertain. The primary outcome was the first‐pass effect (FPE), defined as expanded Treatment in Cerebral Infarction (TICI) 2c/3 on the first pass.
Here are other very interesting posts: Wellens' syndrome: to stent or not? Despite description of Wellens’ Syndrome over 40 years ago — this syndrome remains misunderstood by all-to-many clinicians ( See My Comment at the bottom of the page in the August 12, 2022 post in Dr. Smith’s ECG Blog ).
IntroductionThe accuracy of fenestrations in stent grafts for complex aortic aneurysms and dissections can be significantly improved using three-dimensional (3D)-printed phantoms. Standardization is enhanced by using artificial intelligence (AI) for image pre-processing before 3D printing.
A 60 yo with 2 previous inferior (RCA) STEMIs, stented, called 911 for one hour of chest pain. The first hs troponin I returned at 1100 ng/L Angiogram Lesion on 1st Obtuse Marginal : Proximal subsection = 90% stenosis Stented. He had no h/o heart failure. DBT was 120 minutes, pretty good for a Non-STEMI OMI.
Just before 10 AM, the patient received a stent to the culprit OM. We have discussed repolarization variants on multiple occasions in Dr. Smith's ECG Blog — with detailed description of this entity in the May 23, 2022 post by Dr. McLaren ( Please check out My Comment and illustrative Figure at the bottom of the page of this post ).
Written by Jesse McLaren A 70 year old with prior MIs and stents to LAD and RCA presented to the emergency department with 2 weeks of increasing exertional chest pain radiating to the left arm, associated with nausea. Clin Cardiol 2022 4. The patient was transferred to CCU to consider surgical options. Int J Cardiol 2024 3. Lupu et al.
The cath lab was activated, and then not cancelled, and the angiogram showed 99% TIMI 2 flow proximal LAD culprit lesion, stented in less than 90 minutes of arrival. Cath days later showed complete occlusion of the LAD, stented. Ultimately, cardiac cath was done in Case #2, with stenting of the "culprit" LAD lesion.
LAD and D1 were stented, but flow unfortunately could not be well restored despite efforts (they list the post intervention TIMI flow still as 0). 2022 Jan;51:384-387. 2022 May;55:180-182. 2022 May;55:180-182. Epub 2022 Mar 17. LCX and RCA were described as "normal" in the cath report. Am J Emerg Med. 2021.11.023.
The stent–aspiration (Solumbra) technique uses a large bore aspiration catheter with a stent retriever device for potential synergistic effects. The technique involves deploying a stent retriever through microcatheter and large bore aspiration catheter like ACE 68 (Penumbra, Inc.), years, mean NIHSS 9.1).
Methods:Within 168 FSR-participating hospitals, between January 2010 and September 2022, we analyzed NCIS patients with NIHSS score >3, without other indication(s) for DAPT (e.g., carotid stenting) or systemic anticoagulation, hemorrhagic complications, and whom received at least one antiplatelet agent upon discharge.
Navigation beyond the occlusion and retraction of stent‐retriever/aspiration catheter were the two most common procedural steps that led to perforation.ConclusionIn our cohort, perforation was approximately twice as frequent in MeVO than in LVO thrombectomy. The primary outcomes were independent functional outcome (i.e.
Thus, the QI project aimed to retrospectively examine unexpected or safety events of patients who underwent carotid artery stenting or carotid endarterectomy procedures before versus after implementing the new policy.Objective:To compare and examine the rates of unexpected or safety events that occurred before (5/1/2021 - 10/31/2021; PRE) vs. after (..)
Patients included were of Hispanic origin presenting between 2012 and 2022 who underwent thrombectomy for acute ischemic stroke. vs. 20.5%; p = 0.048) and stenting (28.4% We performed this retrospective cohort analysis to assess the impact of poorly controlled diabetes, defined as HbA1C of 9.0% or greater.
A prehospital “STEMI” activation was called on a 75 year old male ( Patient 1 ) with a history of hyperlipidemia and LAD and Cx OMI with stent placement. It was stented. He wrote most of it and I (Smith) edited. It is also important to recognize that BTWI patterns can be very dynamic. He went to the cath lab at 0900 the next morning.
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chest pain relieved by rest. The reappearance of de Winter's pattern caused by acute stent thrombosis: A case report. Published 2022 Feb 20. As per Drs.
The operator documented thoughtful consideration of risks and benefits of stent placement. Technically, there was a very narrow landing zone for the stent, and missing this could result in "jailing" the LCx, which is ideally avoided. Unfortunately, a few hours later the patient complained of recurrent chest pain.
She was taken to the cath lab, where she was found to have 100% in-stent restenosis of the proximal LAD. For more on Precordial Swirl — See the October 15, 2022 post in Dr. Smith's ECG Blog ). About 45 minutes after the second EKG, the patient was found in cardiac arrest. She was worked as a full code, and ROSC was achieved.
Endovascular devices have catalyzed a global industry for advanced technologies such as flow diverters and stent retrievers. As of April 2022, >85% of 500 000+ previously certified devices were without new certification.In Stroke: Vascular and Interventional Neurology, Ahead of Print.
IntroductionFlow diverters (FD) are stent‐type devices that enable the exclusion of intracranial aneurysms in clinical scenarios where coil‐type devices exhibit high failure rates. Stroke: Vascular and Interventional Neurology, Volume 3, Issue S2 , November 1, 2023. Adults older than 18 with non‐ruptured intracranial aneurysms were included.
We evaluated the impact of IS+ on different efficacy outcome variables: final complete recanalization (eTICI2c-3), total number of passes, procedural duration, and use of bailout technique (angioplasty, stenting, GP2b2a infusion)Results:Of the 200 evaluated patients, 52 (26%) IS+ were found.
MT cases for strokes between 2020 and 2022 were reviewed. To be included, two or more passes of MT using stent retrievers in combination with aspiration must have occurred. Favorable functional outcomes were identified as mRS of 0 to 2 and NIHSS of 0 to 4 at discharge.
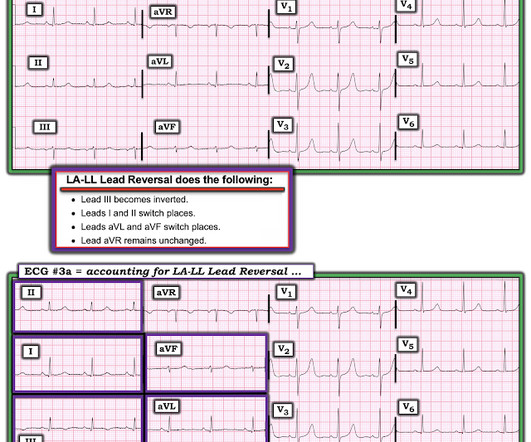
Angiogram: Culprit Lesion (s): Thrombotic occlusion of the proximal RCA -- stented. The April 17, 2022 post ( Leads V1,V2 misplacement ). The May 24, 2022 post ( LA-LL reversal ). The May 26, 2022 post ( LA-LL reversal ). The August 17, 2022 post ( LA-RA reversal ). The November 19, 2020 post ( LA-LL reversal ).
And finally, after placement of a stent in the LAD: Before and after: (Unfortunately, this resulted in the "jailing" of the septal branches behind the stent and probably some degree of plaque shift which is why they do not opacify well in the "after" shot. This was the cost of preventing infarction of the anterior wall.)
The patient is female in her 80s with a medical hx of previous MI with PCI and stent placement. As I discussed in My Comment at the bottom of the page in the April 2, 2022 post in Dr. Smith's ECG Blog — I am aware of many cases of sustained VT in which the patient remained awake and alert for hours.
This led to immediate cath lab activation — which revealed total occlusion of a large 1st diagonal branch that was stented. == Below is the ECG of Patient #3 — recorded from a 35-year old man with sudden, new-onset CP. In a word — Patient #2 was lucky to have his ECG interpreted by the Queen Of Hearts.
The patient was found to have total "mid" LAD occlusion which was stented: Pre-PCI. The October 15, 2022 post in Dr. Smith's ECG Blog features no less than 20 ECG examples by Drs. 25 minutes later, EMS called back with this new ECG: Super obvious STEMI(+) OMI. The cath lab was now activated.
Only 24 patients received intravenous thrombolytics (5.3%) and 47 had stent placement (10.4%). A total of 3 separate groups, low‐dose ticagrelor (45 mg or 60 mg twice a day), full‐dose ticagrelor (90 mg twice a day) and clopidogrel (75 mg daily) were created. Out of 445 patients, 288 were on aspirin 81 mg at time of discharge.
Remember: these findings above are included as STEMI equivalent findings in the 2022 ACC Expert Consensus Decision Pathway on ACS Patients in the ED. Angiogram soon after (around 4 hrs after presentation) showed multi vessel CAD, with culprit lesion total occlusion of the first obtuse marginal branch (OM1), which was stented.
The lesion was successfully stented, but it was unfortunately done after a significant myocardial loss. 2022 Mar-Apr;71:44-46. Epub 2022 Jan 31. PMID: 34523597. == MY Comment by K EN G RAUER, MD ( 11/13/2022 ): == Highly interesting case by Emre Aslanger. References Aslanger EK. J Electrocardiol. 2022.01.006. 2021.21026.
Cath done around 4pm next afternoon: Acute culprit lesion: LCX 99%, TIMI 1 flow, stented Also LAD 50%, TIMI 3 flow, which was also stented And chronic RCA occlusion with collaterals (no information is in the cath report regarding where the collateral flow is from, for example if collateral flow was from the LAD or LCX).
They were stented. 2022 Jan;51:384-387. A DDENDUM ( 2/8/2022 ): Dr. Mario Parrinello , an esteemed cardiology colleague of ours from Cremona, Italy — wrote the following comment regarding today’s post on the EKG Club. [link] Unbeknownst to us at the time, there was an old ECG for comparison from 3.5 Why not very very high?
Stent placed. Increased J-point ST depression, with downslope sagging ST segments and terminal T wave positivity ( ie, markedly positive "Mirror" Test — as per My Comment in the September 21, 2022 post of Dr. Smith's ECG Blog ) — confirms acute posterior OMI. : Now it is not subtle: there is clear, obvious inferior posterior OMI.
Opened and stented. Here are over 30 cases of OMI which was interpretable on the ECG but which the computer called "normal." = Comment by K EN G RAUER, MD ( 12/23 /2022 ): = This is a “quickie case” that I like — because it reinforces a series of KEY principles essential to rapid decision-making.
Compare to the anatomy after stenting: The lower of the 2 now easily seen branches is the circumflex, now with excellent flow. 2022 Mar-Apr;71:44-46. Epub 2022 Jan 31. Comment by K EN G RAUER, MD ( 12/18 /2022 ): = Important case with numerous diagnostic Pearls presented by Dr. Aslanger. The patient recovered well.
The 50-something patient with history of coronary stenting and slightly reduced LV ejection fraction. In the setting of prior stenting and reduced left ventricular ejection fraction, would pursue a heart team revascularization approach Syntax score 28.5, This alone could be due to LVH, but V4 could NOT be due to LVH.
Angiogram found a totally occluded first diagonal artery, consistent with all the ECGs, which reperfused after stenting. But there were no more ECGs for the next 8 hours before angiogram, and no further troponin levels for the remainder of the patient’s admission. This is usually a result of restoration of flow from collaterals.
This middle aged male with h/o GERD but also h/o stents presented to the ED with chest pain. He had been at a clinic that day where he had complained of worsening GERD. An EKG was reco rded and interpreted as normal by the computer, the clinician, and by the overreading cardiologist.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
















































Let's personalize your content