This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
A 60 yo with 2 previous inferior (RCA) STEMIs, stented, called 911 for one hour of chest pain. Here is his most recent previous ECG: This was recorded after intervention for inferior STEMI (with massive ST Elevation, see below), and shows inferior Q-waves with T-wave inversion typical of completed inferior OMI.
Written by Jesse McLaren A 70 year old with prior MIs and stents to LAD and RCA presented to the emergency department with 2 weeks of increasing exertional chest pain radiating to the left arm, associated with nausea. I sent this to the Queen of Hearts So the ECG is both STEMI negative and has no subtle diagnostic signs of occlusion.
The interventional cardiologist then canceled the activation and returned the patient to the ED without doing an angiogram ("Not a STEMI"). I advised that perhaps posterior leads would help to persuade the interventionalist, since the 2022 ACC recommendations include posterior STEMI as a formal STEMI equivalent, but only officially by 0.5
The lesion was successfully stented. Take home messages: 1- In STEMI/NSTEMI paradigm you search for STE on ECG. If this patient was managed according to the STEMI/NSTEMI paradigm (although he would be a candidate for early invasive treatment), he would probably be taken to the cath lab hours later. Turk Kardiyol Dern Ars.
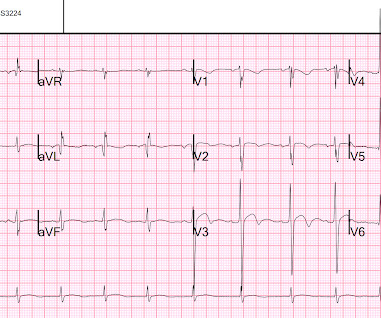
Notice on the right side of the image how the algorithm correctly measures STE sufficient in V1 and V2 to meet STEMI criteria in a man older than age 40. As most would agree, this ECG shows highly specific findings of anterolateral OMI, even with STEMI criteria in this case. Thus, this is obvious STEMI(+) OMI until proven otherwise.
Patient still not having chest pain however this is more concerning for OMI/STEMI. Wellens' syndrome is a syndrome of Transient OMI (old terminology would be transient STEMI). As far as I can tell, there is only one randomized trial of immediate vs. delayed intervention for transient STEMI. Labs ordered but not yet drawn.
Subtle as a STEMI." (i.e., She was taken to the cath lab, where she was found to have 100% in-stent restenosis of the proximal LAD. In our study, there were 20/53 complete LAD OMI (TIMI-0 flow) which did not meet STEMI criteria. None of the 20 ever evolved to STEMI criteria. This one is easy for the Queen.
A prehospital “STEMI” activation was called on a 75 year old male ( Patient 1 ) with a history of hyperlipidemia and LAD and Cx OMI with stent placement. The two cases were considered: Patient 1 was recognized by the ED provider and the cardiologist as having resolved “STEMI”. It was stented. This was a large OMI.
Here they are: Patient 1, ECG1: Zoll computer algorithm stated: " STEMI , Anterior Infarct" Patient 2, ECG1: Zoll computer algorithm stated: "ST elevation, probably benign early repolarization." He diagnosed anterior "STEMI" and activated the cath lab. 25 minutes later, EMS called back with this new ECG: Super obvious STEMI(+) OMI.
This is documented as a STEMI in the clinical notes and in the cath report, but certainly does not meet STEMI criteria and is therefore an NSTEMI by definition. For national registry purposes, this will be incorrectly classified as a STEMI.) Most STEMI have peak cTnI greater than 10.0. Large STEMI are approximately 30-80.
Recall from this post referencing this study that "reciprocal STD in aVL is highly sensitive for inferior OMI (far better than STEMI criteria) and excludes pericarditis, but is not specific for OMI." Here is the angiogram after stent placement. Immediate versus delayed invasive intervention for non-stemi patients. Marinkovic, J.,
There is an obvious inferior posterior STEMI(+) OMI. Angiogram: Culprit Lesion (s): Thrombotic occlusion of the proximal RCA -- stented. Results Of 149 patients with inferior STEMI , 43 (29%) had RVMI and 106 (71%) did not. What is the atrial activity? Is it sinus arrest with junctional escape? How would one tell?
The cath lab was activated, and then not cancelled, and the angiogram showed 99% TIMI 2 flow proximal LAD culprit lesion, stented in less than 90 minutes of arrival. Cath days later showed complete occlusion of the LAD, stented. Another missed OMI by the False STEMI-NonSTEMI Dichotomy Don't miss them!!! Normal vitals.
P.S.: Cardiac cath was performed — and showed a distal LA D "culprit" lesion that was successfully stented. It may look identical t o the ST-T wave appearance seen after a STEMI with marked troponin elevation, that has now reperfused ( be this reperfusion spontaneous — or by treatment with PCI or thrombolytics ).
Step 1 to missing posterior MI is relying on the STEMI criteria. A prospective validation of STEMI criteria based on the first ED ECG found it was only 21% sensitive for Occlusion MI, and disproportionately missed inferoposterior OMI.[1] But it is still STEMI negative. A 15 lead ECG was done (below). In a study last year, 14.4%
But because there was no new ST elevation, the ECG was signed off as “STEMI negative” and the patient waited to be seen. But the ECG still doesn’t meet STEMI criteria. It was therefore interpreted as “no STEMI” and the patient was treated with dual anti-platelets and referred to cardiology as “NSTEMI.” the cardiologist 5.
Unfortunately, the cardiologist waited until the next day to refer the patient for angiography and intervention because patient did not meet criteria for "STEMI"." Successful primary angioplasty of the mid-circumflex artery towards the main marginal branch with the implantation of a drug-eluting stent. Good angiographic result.
Since then, I started looking for OMI EKG findings and not just STEMI. Remember: these findings above are included as STEMI equivalent findings in the 2022 ACC Expert Consensus Decision Pathway on ACS Patients in the ED. mm in lead I, thus not STEMI criteria) and was finally understood by the cardiologist.
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chest pain relieved by rest. The reappearance of de Winter's pattern caused by acute stent thrombosis: A case report. Published 2022 Feb 20. As per Drs.
Code STEMI was activated by the ED physician based on the diagnostic ECG for LAD OMI in ventricular paced rhythm. This was several months after the 2022 ACC Guidelines adding modified Sgarbossa criteria as a STEMI equivalent in ventricular paced rhythm). LAFB, atrial flutter, anterolateral STEMI(+) OMI. Limkakeng AT.
While this ECG is negative for “posterior STEMI”, the resolution of anterior ST depression (accompanied by the troponin elevation) confirms posterior OMI with spontaneous reperfusion. The second opportunity to make the diagnosis and expedite angiography was missed because the ECG never met STEMI criteria and continued to be labeled ‘normal.’
It definitely does not fulfill STEMI criteria, and I would argue that it would not lead to cath lab activation in most centers. As a result, this 45-year old man did not experince any delay in treatment — and a large diagonal branch of the LAD was stented with good outcome. To the uninitiated — this ECG may appear normal.
They were stented. 2022 Jan;51:384-387. These include about 60 occlusion MI (OMI) with clear ST segment elevation (none of which would be called “Normal” by the computer) and about 165 Non-STEMI. Of the Non-STEMI in our cohort, about 25% will actually have acute coronary occlusion. The peak troponin was 1863 ng/L.
Opened and stented. This is why it is essential that the OMI/NOMI paradigm replace the STEMI/NonSTEMI paradigm. Under Non-STEMI, this patient would not have intervention until at least 20 hours (next day), after the infarct is completed. Angiogram: Occlusion of branch of First Obtuse Marginal. Learning Points: 1.
Later, she developed chest pain again, and had this ECG recorded: Obvious Anterior OMI that is also a STEMI Coronary angiogram- --Right dominant coronary artery system --The left main artery was normal in appearance and free of obstructive disease. --The Thus, Wellens' syndrome should be thought of as a transient OMI or transient STEMI.
The lesion was successfully stented, but it was unfortunately done after a significant myocardial loss. 2022 Mar-Apr;71:44-46. Epub 2022 Jan 31. PMID: 34523597. == MY Comment by K EN G RAUER, MD ( 11/13/2022 ): == Highly interesting case by Emre Aslanger. References Aslanger EK. J Electrocardiol. 2022.01.006. 2021.21026.
Diagnosis: Acute non-ST segment elevation MI (Non-STEMI, or NSTEMI) Second troponin returned at around 0200: 15,894 ng/L 0245 (unclear if ongoing pain or not) Inferoposterior (and lateral V5-6) reperfusion findings. Admitted to the hospital service for further evaluation and management." No further ECG were ever recorded.
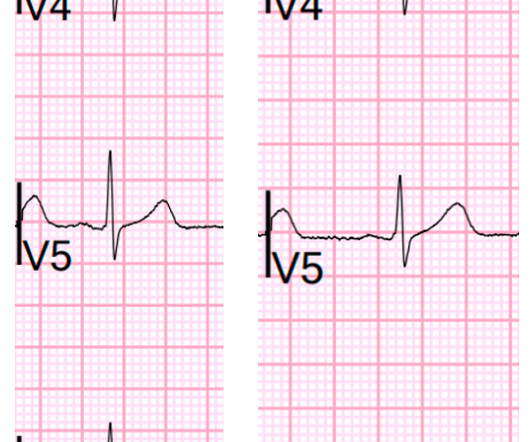
The 50-something patient with history of coronary stenting and slightly reduced LV ejection fraction. In the setting of prior stenting and reduced left ventricular ejection fraction, would pursue a heart team revascularization approach Syntax score 28.5, This alone could be due to LVH, but V4 could NOT be due to LVH.
He was taken to the cath lab where he was found to have acute total occlusion of his saphenous vein graft to his RCA, which was stented. His second troponin was 46 ng/L. No further troponins were measured. He was in cardiogenic shock requiring an impella for several days after cath. Such is the situation in today's post by Drs.
Compare to the anatomy after stenting: The lower of the 2 now easily seen branches is the circumflex, now with excellent flow. 2022 Mar-Apr;71:44-46. Epub 2022 Jan 31. Comment by K EN G RAUER, MD ( 12/18 /2022 ): = Important case with numerous diagnostic Pearls presented by Dr. Aslanger. The patient recovered well.
Immediate and early percutaneous coronary intervention in very high-risk and high-risk Non-STEMI patients. Clin Cardiol 2022; [link] Labs included: hsTnI 156 ng/L, Hb 12 g/dL, WBC 12x10^9/L, Cr. A single DES stent was placed, and the patient did well post-procedure. Lupu L, et al. mg/dL, K 3.5
Note: according to the STEMI paradigm these ECGs are easy, but in reality they are difficult. Theres inferior STE which meets STEMI criteria, but this is in the context of tall R waves (18mm) and relatively small T waves, and the STD/TWI in aVL is concordant to the negative QRS. This was false positive STEMI with an ECG mimicking OMI.
He reports this was similar to how he felt when he had his heart attack 4 years prior, now s/p 4 stents. Note: the 2022 ACC Expert consensus Chest pain guidelines state that "posterior STEMI-Equivalent" is a sign of acute coronary occlusion. 2/3 of STEMI have a peak 4th generation troponin I greater than 10.0
Case submitted by Andrew Grimes, Advanced Care paramedic, with additions from Jesse McLaren and Smith An 84-year-old male with a notable cardiac history (CABG, multiple stents) woke at 0500hrs with pressure in his chest, diaphoresis, and light-headedness. STEMI criteria are only 43% sensitive for OMI.
He had undergone stenting of the LAD several weeks ago (unclear whether elective for stable symptoms, or in response to acute coronary syndrome). Acute chest pain, right bundle branch block, no STEMI criteria, and negative initial troponin. Written by Pendell Meyers An adult man presented with acute chest pain.
He has a history of coronary artery disease and a STEMI two years prior that was treated with primary PCI. At the time of this initial ED ECG, his symptoms were improving ECG #1 on admission to the ED The patient was not seen quickly in the ED as it was a busy shift and the ECG did not meet STEMI criteria. The below ECG was recorded.
Here is the prehospital ECG, recorded in the presence of pain: Hyperacute anterolateral STEMI The medics had activated the cath lab and the patient went for angiogram and had a 95% stenotic LAD with TIMI-3 flow. A stent was placed. Serial ECGs demonstrated dynamic changes diagnostic of ACS (transient STEMI) 4.
After stent deployment, we often see improvement in the ST-T within seconds or minutes. Here is the final angiogram following placement of a stent in the ostial RCA. 2:04 PM, post stent deployment You can see that even after complete restoration of flow, the ECG still looks terrible, V most of all. link] Bai, J., Tang, Z., &
At 1210, the case was discussed with a cardiologist at a PCI capable facility, who accepted the patient for transfer, noting the ST depression in anterior leads as consistent with ischemia but not a STEMI. The proximal and mid LAD stenoses were stented and the OM 2 was left alone. 5 years later ( now in 2025 ) the problem remains.
The first EKG was concerning for a Wellen’s-like pattern of subtle reperfusion changes in the setting of stuttering anginal-equivalent symptoms, but none were diagnostic of STEMI or OMI. Later in the night, the patient became bradycardic and developed a Mobitz II pattern , but he remained asymptomatic and hemodynamically stable.
It is diagnostic of OMI, but this is SUBACUTE OMI I sent this ECG to my "EKG Nerdz" friends, without any clinical info at all and they answered "OMI" The Queen said: "STEMI-Equivalent with High Confidence:" Notice she sees findings in both normal beats and PVCs. It was opened and stented. There are new Q-waves in aVL, V5-6.
At cath later the same day, a proximal 99% RCA culprit lesion was stented. Following the improvement in the ECG the patient's pain too improved drastically. This of course proves that the initial ECG was OMI and that the artery has reperfused. Troponin T peaked at 4051 ng/L. The difference is only 30 degrees and up to 45 degrees is normal.
The cath lab was deactivated by cardiologist on arrival at ED because it was "not a STEMI". First obtuse marginal also had an 80% stenosis and was stented. 2022;Available from: [link] Click here to sign up for Queen of Hearts Access. == MY Comment, by K EN G RAUER, MD ( 10/27/2024 ): == I view today's case as unfortunate.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
















































Let's personalize your content