This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
The most accurate way (But not the only way) to answer this question is whether or not you have plaque in your coronary arteries. If you already have plaque, your risk of event an event goes up proportional to the amount of plaque you have 2. In this scenario, your risk of a heart attack over the next 10 years is well under 2%.
Anthos subsequently kicked off three phase 3 trials in 2022, and wrapping up these studies by 2026 will now be Novartis responsibility. Besides the hefty price tag , the re-acquisition puts Novartis back into competition with other big-name Factor XI inhibitor developers, whove faced a series of setbacks.
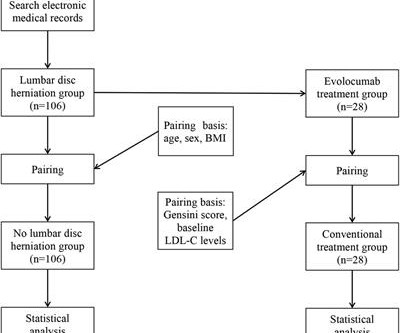
Objective Assessing the impact of lumbar disc herniation (LDH) on the plaque burden of coronary atherosclerosis is our objective. Methods In this study, a total of 212 patients (age 46–80 years) with unstable angina (UA) who underwent coronary angiography (CAG) in our hospital from January 2018 to July 2022 due to UA were included.
You cannot eliminate the plaque entirely, but multiple clinical trials have shown plaque regression using high-intensity cholesterol-lowering treatments, which I have discussed previously. All of these parameters are important and need to be considered when evaluating plaque regression. REVERSAL Investigators.
Thus, it has recently become generally accepted that most plaque ruptures resulting in myocardial infarction occur in plaques that narrow the lumen diameter by 40% of the arterial cross section may be involved by plaque. The pathologist may see a plaque that constitutes, for example, 50% of the cross-sectional area.
Background:High-risk non-stenosing carotid plaque features are emerging as a possible source of embolism in the setting of ESUS. We utilized Fisher’s exact test to compare the frequencies of reporting each plaque characteristic.Results:We analyzed 152 CTA reports in depth.
BackgroundComplex aortic plaque (CAP) is a potential embolic source in patients with cryptogenic stroke (CS). Most studies (74%) used ≥4 mm plaque thickness as the imaging criterion for CAP although ≥1 mm (N=1, CTA), ≥5 mm (N=5, TEE), and ≥6 mm (N=2, CTA) were also reported. 0.41],I2=94%). I2=95%) for TEE; 0.23 (95% CI, 0.15–0.34;I2=87%)
Lp(a) is emerging as an important, yet under-recognized, potential risk factor for cardiovascular disease due to its ability to promote the development of plaques within artery walls, clot formation and aortic valve calcification. 2022 Aug, 80 (9) 934946 Kronenberg F.
Carotid ultrasound results were divided into two groups based on the presence or absence of plaque. Carotid plaque was observed in 1140 (43.5%) subjects and CACS>0 in 1172 (44.7%) subjects. Carotid plaque was observed in 1140 (43.5%) subjects and CACS>0 in 1172 (44.7%) subjects. 1692 (64.6%) were male.
Carotid plaque (CP) is an independent risk factor for cardiovascular diseases. However, evidence for association of MHR with risk of CP is scarce.Methods and ResultsThis study involved 5260 participants aged >18 years old from the Dalian health management cohort in 2014 to 2022.
Materials and methods This retrospective, institutional-review board approved study included consecutive patients with calcified coronary artery plaques undergoing CCTA with PCD-CT and invasive coronary angiography between July and December 2022. Virtual monoenergetic images (VMI) and VNCa images were reconstructed.
This is because the test is widely available, fast, highly reproducible, low radiation, directly reflective of total coronary plaque burden, and highly predictive of future atherosclerotic cardiovascular disease (ASCVD) events.
A heart attack is when that plaque ruptures and stops blood flow down the artery. 2022 Mar 14. The pathology that causes heart disease (atherosclerosis) is, by definition, the abnormal retention of a cholesterol particle in the artery wall. Cholesterol is an essential part of that process. But other factors also play a role.
Non-obstructive coronary disease at the time cardiac cath is done does not necessarily imply there was no plaque rupture with thrombus. These plaques will often not be recognized as "culprits" — because no fissuring or ulceration is seen.
Overall healthcare AI clearances are gaining momentum, with 2023 bringing a 42% jump in clearances, more than doubling 2022 and 2021’s annual growth (+20% & +16%). FFRCT, coronary plaque, etc). in 2020-2022, and 13.5% Cardiovascular AI actually makes up a larger 17.4% since the start of 2023.
MINOCA may be due to: coronary spasm, coronary microvascular dysfunction, plaque disruption, spontaneous coronary thrombosis/emboli , and coronary dissection; myocardial disorders, including myocarditis, takotsubo cardiomyopathy, and other cardiomyopathies. Thus, intracoronary imaging modalities are crucial in this setting. From Gue at al.
The Award will refer to articles published in 2021 and 2022. The Award will be given to the Brazilian authors of the best Original Article published in the ABC Cardiol and IJCS journals for the years 2021 and 2022, and to Brazilian authors of the best Original Article published in the ABC Imagem and ABC HF journals in 2022.
Angiography : --Culprit for the patient's unstable angina/Wellen syndrome is a ruptured plaque in the mid LAD. --As Despite description of Wellens’ Syndrome over 40 years ago — this syndrome remains misunderstood by all-to-many clinicians ( See My Comment at the bottom of the page in the August 12, 2022 post in Dr. Smith’s ECG Blog ).
Atherosclerotic cardiovascular disease (ASCVD), caused by plaque buildup in arterial walls, is one of the leading causes of disability and death worldwide.1,2 7 Research has shown inflammation plays a significant role in the development of atherosclerosis and ASCVD,8-10 and even the formation of plaque.11 2022 Sep 6;146(10):e141].
His ECG at the accepting facility is shown below: Accepting facility ECG The team reviewed his angiography films with an interventionalist and thought they were suspicious for plaque rupture in LAD, but they were not confident.
A CTCA provides much more anatomical detail and can identify advanced plaque often missed by CT Coronary Artery Calcium Score scans alone. There are 3 types of coronary atherosclerosis visible on CTCA: Calcified Plaque - Easily Identified on both CT CAC & CTCA scans. Subscribe now How Often Does A CT CAC Scan Miss Plaque?
Detailed analysis of the excised carotid plaques were carried out with pyrolysis-gas chromatography-mass spectrometry, stable isotope analysis, and electron microscopy. Primary endpoint of the study was a composite of myocardial infarction, stroke, or death from any cause in those who had micro and nanoplastics in the carotid plaque.
There will be an award for the most cited national manuscript in the last two years, namely: the most cited article published in 2021 and 2022 in 2023, for the journals ABC Cardiol and IJCS; and the most accessed in 2023 for the journals ABC Imagem and ABC HF. Awards granted: a) Plaque for each awarded article.
With Plaque Features Associated with False Positives. AJR Am J Roentgenol 2022 Sep;219(3):407-419. Presented at the European Association of Cardiovascular Imaging: Late Breaking Clinical Research and Trials. Barcelona, Spain. 4 Chiou A, Hermel M, Miller G et al. 7 Bär S, Nabeta T, Maaniitty T.
The incidence of no-reflow was higher in patients with attenuated plaque ≥5 mm in length as evaluated by intravascular ultrasound (IVUS).Objective:The The incidence of no-reflow was higher in patients with attenuated plaque ≥5 mm in length as evaluated by intravascular ultrasound (IVUS).Objective:The vs. 8.6%, p < 0.001).
Smith comment : a very high proportion of MINOCA are ruptured plaque with lysed thrombus. That plaque is at risk of thrombosing again. It is worthwhile remembering that the majority of plaques which rupture are non-obstructive before they ulcerate and thrombose. Most plaque is outside the lumen!!
5 High intensity interval training induces beneficial effects on coronary atheromatous plaques – a randomized trial, European Journal of Preventive Cardiology , 2022;, zwac309, 6 FOURIER Steering Committee and Investigators. 2006 Apr 5;295(13):1556-65. Evolocumab and Clinical Outcomes in Patients with Cardiovascular Disease.
This study aimed to determine the current prevalence of CAS and examine the associated gender differences in adults.Methods:From September 2021 to June 2022, we established a prospective cohort to study CAS and cardiovascular disease across 25 project sites in Henan, China, utilizing a multistage whole-population sampling method.
J Electrocardiol [Internet] 2022;Available from: [link] Cardiology opinion: Takotsubo Cardiomyopathy (EF 30-35%) V Fib Cardiac arrest Prolonged QTC NSTEMI (Smith comment: is it NSTEMI or is it Takotsubo? -- these are entirely different) Moderate single-vessel CAD. An angiogram is a "lumenogram;" most plaque is EXTRALUMINAL!!
FFRCT, coronary plaque, echo AI, etc)… We’re using this broader definition of cardio AI through the rest of this story. Cardiovascular AI’s total share of H1 2024 AI clearances was the highest since 2020 (both 18%), after landing between 14% and 16% during the last three years.
The complications of the procedure and patient’s outcomes were discussed.MethodsWe identified two patients who were admitted to our medical center between January 2022 to December 2022 for subclavian‐carotid artery bypass procedure. Clinical data were reviewed retrospectively.ResultsCase 1.
It is generally believed it is more of a mechanical plaque lesion. BMC Cardiovasc Disord 22 , 176 (2022). RCA and LCX Wellens do occur, making this entity’s perceived unique importance less certain 3. How common is thrombosis in the culprit artery of Wellen syndrome ? However by no means, we can say thrombosis do not occur.
The aim is to highlight distinguishing features of CAD on VW-MRI, demonstrating its ability to offer better visualization of vessel wall abnormalities in select cases compared to conventional CTA.Methodology:Patients were selected from the University of Washington (UW) hospital system between 2022 and 2024.
While the total body seems to do little in determining cholesterol levels, what is more scientifically shocking is slope of the curve between blood LDL levels and plaque burden is rarely linear. Nat Cardiovasc Res 1 , 554–561 (2022). LDL is obviously a target against atherosclerosis. Mind you LDL constitutes.000025% Reference 1.Lib
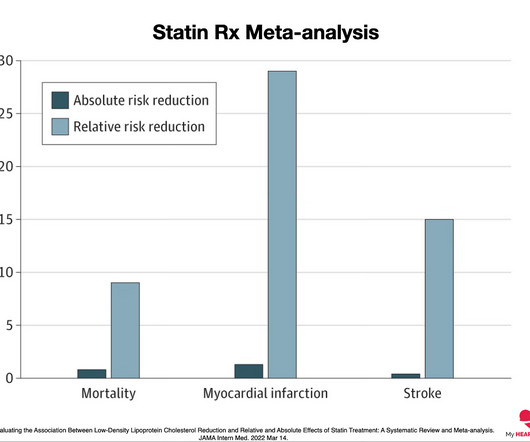
26th August 2022 And so, after a great deal of faffing about, my article on cardiovascular disease ‘Assessing cardiovascular disease: looking beyond cholesterol’ has been made free to view. A study in JAMA in 2022 suggested that ‘the absolute benefits of statins are modest and may not be strongly mediated through the degree of LDL reduction’.
24: Joint American College of Cardiology/Journal of the American College of Cardiology Late-Breaking Clinical Trials (Session 402) Saturday, April 6 9:30 – 10:30 a.m.
Reperfusion of OMI indicates at least partial thrombolysis of occluding thrombus, but still unstable plaque rupture, which can reocclude at any moment. Comment by K EN G RAUER, MD ( 12/14 /2022 ): = We've reviewed many cases that illustrate the challenge posed by distinguishing between marked LVH — vs — LVH + superimposed acute OMI.
And finally, after placement of a stent in the LAD: Before and after: (Unfortunately, this resulted in the "jailing" of the septal branches behind the stent and probably some degree of plaque shift which is why they do not opacify well in the "after" shot. This was the cost of preventing infarction of the anterior wall.) ng/mL (ref.
Therefore it means acute type 1 ACS plaque rupture with impeded flow and impending full occlusion until proven otherwise. Published 2022 Feb 20. 2022;Available from: [link] 7. Then, the patients third ECG showed a very rare combination of de Winter T waves happening during LBBB. Hayakawa A, Tsukahara K, Miyagawa S, et al.
Acute MI due to plaque rupture does happen in young people, including young women. It is only meaningful if you can accurately interpret the ECG. Here are 11 cases of young women with acute MI. Beware when the computer calls the ECG "normal." It is not unusual for the initial Troponin value to be normal.
Routine STEMI activation in STE-aVR for emergent revascularization is not warranted, although urgent, rather than emergent, catheterization appears to be important. == MY Comment, by K EN G RAUER, MD ( 11/4 /2022 ): == Our thanks to Drs.
The coronary angiogram revealed no critical stenosis, or acute plaque ulceration. Surawicz and Knilans report that intense catecholamine surge, or severe maladjustment of the autonomic nervous system, can manifest “cerebral T waves” in the absence of an acute intracranial process. Furthermore, pertinent electrolyte values (e.g. Saini, A.,
As in all ischemia interpretations with OMI findings, the findings can be due to type 1 AMI (example: acute coronary plaque rupture and thrombosis) or type 2 AMI (with or without fixed CAD, with severe regional supply/demand mismatch essentially equaling zero blood flow). This patient arrested shortly after hospital arrival.
The ECG is diagnostic for acute transmural infarction of the anterior and lateral walls, with LAD OMI being the most likely cause (which has various potential etiologies for the actual cause of the acute coronary artery occlusion, the most common of which is of course type 1 ACS, plaque rupture with thrombotic occlusion).
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.











































Let's personalize your content