This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
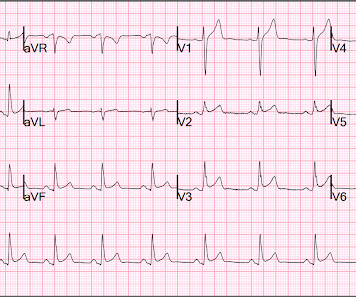
The patient was discharged with a diagnosis of acute pericarditis — and treated with a full course of colchicine and ibuprofen. The ultimate discharge diagnosis was acute pericarditis. ( From the information provided — I would not make the diagnosis of acute pericarditis. Figure-1: The initial ECG in today's case.
Overall, this looks like one of the rare ECGs that is actually specific for pericarditis in my opinion. Pericarditis maybe." Meyers' words — "is one of the rare ECGs that is actually specific for pericarditis". ii ) Today's case emphasizes the importance of the history in making the diagnosis of pericarditis.
Background There are limited data on acute pericarditis according to different age groups. The aim of this study is to investigate the role of age-related features in clinical characteristics, management, and outcomes of acute pericarditis, with a focus on the geriatric population. Results A total of 471 patients (median age 56.3 (IQR
This is a value typical for a large subacute MI, n ormal value 48 hours after myocardial infarction is associated with Post-Infarction Regional Pericarditis ( PIRP ). As already mentioned, this patient could have post-infarction regional pericarditis from a large completed MI. Sinus tachycardia has many potential causes. Hammill SC.
The undergraduate continues: This new EKG pattern is more suggestive of acute pericarditis. Usually with pericarditis, some degree of PR segment depression is expected. This is typical of pericarditis. But, as I always say, you diagnose pericarditis at your peril. This EKG seems to lack it.
Inferior hyperacute T waves, which have been added to the 2022 ACC consensus on chest pain as a “STEMI equivalent”[3] 3. 2022 ACC expert consensus decision pathway on the evaluation and disposition of acute chest pain in the emergency department: a report of the American College of Cardiology solution set oversight committee.
The case reports Case 1 involves a 26 year old man who developed pericarditis after the Pfizer vaccine. Pericarditis, an inflammation of the sac the heart lives in, developed about 7 days after the Pfizer vaccine. The diagnosis was made based on classic findings of inflammation on an electrocardiogram associated with acute chest pain.
ECG of pneumopericardium and probable myocardial contusion shows typical pericarditis Male in 30's, 2 days after Motor Vehicle Collsion, complains of Chest Pain and Dyspnea Head On Motor Vehicle Collision. Retrieved July 2, 2022, from [link] Moyé, D. Retrieved July 2, 2022, from [link] Sybrandy, K. ST depression. Zangouri, V.,
2022 Jul;27(4):e12939. Epub 2022 Feb 11. I last reviewed the phenomenon of electrical alternans in My Comment at the bottom of the page in the November 28, 2022 post of Dr. Smith's ECG Blog. Prolonged ST segment and T-wave alternans with torsade de pointes secondary to hypocalcemia due to hypoparathyroidism: A case report.
These latter findings are typical of pericarditis, but pericarditis never has reciprocal ST depression. Usually with pericarditis and myocarditis — hyperacute T waves (HATW) are not present. S mith : there is STE in lead III and reciprocal STD in aVL. This is OMI until proven otherwise.
First, many on Twitter said "Pericarditis". This is NOT pericarditis, which virtually NEVER has ST depression any where except aVR. See our publication: ST depression in lead aVL differentiates inferior ST-elevation myocardial infarction from pericarditis There is STE in inferior leads, high lateral leads, and V4-V6.
This is a bad ST vector orientation, because it causes widespread STE and one of the most important mistakes that needs to be avoided here is thinking of the diagnosis of pericarditis. Such an out-of-proportion STE is virtually never seen in pericarditis. 2022 Mar-Apr;71:44-46. Epub 2022 Jan 31. References Aslanger EK.
Of course the patient was saddled with the erroneous "pericarditis" diagnosis after CTs ruled also ruled out PE and dissection. The October 15, 2022 post in Dr. Smith's ECG Blog features no less than 20 ECG examples by Drs. Serial ECGs remained unchanged. But he did well.
You can easily imagine this patient getting one of several diagnoses -- vasospasm, MINOCA , pericarditis, or maybe even no diagnosis at all beyond "non-obstructive coronary artery disease." NOTE: For review of 20 cases of "Swirl" vs Swirl "Look-Alikes" — Check out the October 15, 2022 post in Dr. Smith's ECG Blog.
ECG of pneumopericardium and probable myocardial contusion shows typical pericarditis Male in 30's, 2 days after Motor Vehicle Collsion, complains of Chest Pain and Dyspnea Head On Motor Vehicle Collision. I've copied KEY points from My Comment in the August 6, 2022 post in Dr. Smith's ECG Blog — regarding the answer to this question.
Assessment:" " Nonspecific ST elevation from V1-V4 , question of early repolarization versus pericarditis , question of acute current of injury and ? Pericarditis would be even more unlikely in someone without chest pain. Precordial Swirl in ECG #1: As discussed in the October 15, 2022 post in Dr. Smith's ECG Blog — Drs.
The second most common cause of medical cardiac tamponade is acute idiopathic pericarditis. Less common etiologies include uremia, bacterial or tubercular pericarditis, chronic idiopathic pericarditis, hemorrhage, and other causes such as autoimmune diseases, radiation, myxedema, etc. As per Drs.
Here is the South African Flag sign ( Figure by Ken Grauer — with the original 12-lead from Patient 1 attached below — See his Comment from the April 8, 2022 post in Dr. Smith's ECG Blog for more on this sign ). Patient 2 has a normal variant ECG which mimics high lateral OMI, and ruled out for MI, see case below.
Further Reading: [link] See these relevant cases: A man in his 50s with acute chest pain and diffuse ST depression "Pericarditis" strikes again Is it important to recognize LVH Pseudo-infarction patterns?
Traditionally used as an anti-inflammatory for pericarditis (inflammation of the lining of the heart), it has recently been shown to result in fewer major heart events in those with a recent heart attack. JACC Volume 79, Issue 17 , 3 May 2022, Pages 1690-1700 9 Semaglutide and Cardiovascular Outcomes in Obesity without Diabetes.
Pericarditis? If you were thinking that this is pericarditis, that would be possible in the absence of any clinical information. However, there is zero PR depression which would be VERY unusual in pericarditis. P.S.: Acute pericarditis may produce diffuse ST elevation. Presence of STD is helpful; absence is not.
Recall from this post referencing this study that "reciprocal STD in aVL is highly sensitive for inferior OMI (far better than STEMI criteria) and excludes pericarditis, but is not specific for OMI." St depression in lead AVL differentiates inferior st-elevation myocardial infarction from pericarditis. link] Bischof, J. Worrall, C.,
They include myocardial ischemia, acute pericarditis, pulmonary embolism, external compression due to mass over the right ventricular outflow tract region, and metabolic disorders like hyper or hypokalemia and hypercalcemia. 2022 Mar;8(3):386-405. According to a recent systematic review and meta-analysis, spontaneous type 1 ECG had 2.4%
The initial computer and final cardiology interpretation was a differential: “ST elevation, consider early repolarization, pericarditis, or injury.” But STEMI criteria ignore all this and look at ST segments in isolation. Based on STEMI criteria and unhelpful computer interpretation, the patient was rushed to the cath lab.
The "flu-like" illness suggests myo- or pericarditis, but that would be a diagnosis of exclusion. The October 21, 2022 post — for " artifactual VT". A bedside ultrasound should be done to assess volume and other etiologies of tachycardia, but if no cause of type 2 MI is found, the cath lab should be activated NOW. The case continues.
Dyspnea, Chest pain, Tachypneic, Ill appearing: Bedside Cardiac Echo gives the Diagnosis 31 Year Old Male with RUQ Pain and a History of Pericarditis. NOTE: For more on the ECG diagnosis of acute RV "strain" ( and acute PE ) — Please check out My Comment at the bottom of the page in the March 28, 2022 post in Dr. Smith's ECG Blog.
First Troponin I was <2 and peak was 8, echo showed subtle apical lateral hypokinesis, CRP was elevated, and patient was discharged with a diagnosis of regional pericarditis. In this case, there would be evolution, but the evolution would be typical of pericarditis (if the diagnosis of pericarditis was accurate!!
Though less prevalent in younger patients, occlusion MI may occur and requires the same early interventions as older patients. - - Pericarditis and myocarditis should be a diagnosis of exclusion. I've listed potential causes of acute pericarditis in My Comment at the bottom of the page in the June 11, 2022 post in Dr. Smith's ECG Blog.
The exception is with postinfarction pericarditis , in which a completed transmural infarct results in inflammation of the subepicardial myocardium and STE in the distribution of the infarct, and which results in increased STE and large upright T-waves. These findings together are more commonly seen with pericarditis.
Prominent J waves and ventricular fibrillation caused by myocarditis and pericarditis after BNT162b2 mRNA COVID-19 vaccination. Can J Cardiol 2022 Kukla P, Jastrezebski M, Praefort W. This is the 2nd ECG from the February 8, 2022 post in Dr. Smith's ECG Blog ). Internat J Arrhyth 2020 Uesako H, Fukikawa H, Hashimoto S, et al.
The ‘post-vaccination’ cohort comprised vaccinated patients with CHD and matched controls with first-recorded SARS-CoV-2 infection between 1 March 2021 and 1 April 2022, at least 14 days after vaccination (57 550 cases, 225 160 controls). Odds of severe COVID-19 outcomes were compared using conditional logistic regression.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




































Let's personalize your content